- Written By: Sonja Poole, PGY2 FM – Yellowknife NWT
- Reviewed By: Dr Andrew Kotaska OBGYN, – Yellowknife NWT
Some definitions:
- Infertility = inability to conceive or carry to term after 1 year of regular, unprotected intercourse
- Primary infertility = infertility in the context of no prior pregnancies
- Secondary infertility = infertility in the context of a prior conception
As a disclaimer, we are going to be heteronormative with our language to simplify referring to the person providing the sperm as the male partner and the person providing the ovum as the female partner, and using cis-gendered pronouns. This is because those are the two essential ingredients for producing an embryo and they both have specific health considerations.
People who are non-binary, trans, or in queer relationships may also struggle with infertility. Referring to people by their preferred pronouns is extremely important and separating our ideas of sex and gender identity is crucial to providing excellent care. Keep this in mind as you listen to this episode.
Case:
you’re working in a family practice clinic in your community. Shelley, a 34-year-old accountant, comes to see you to talk about family planning. Her and her husband Mike have been trying to get pregnant for the first time and have not had any luck yet.
Objective One

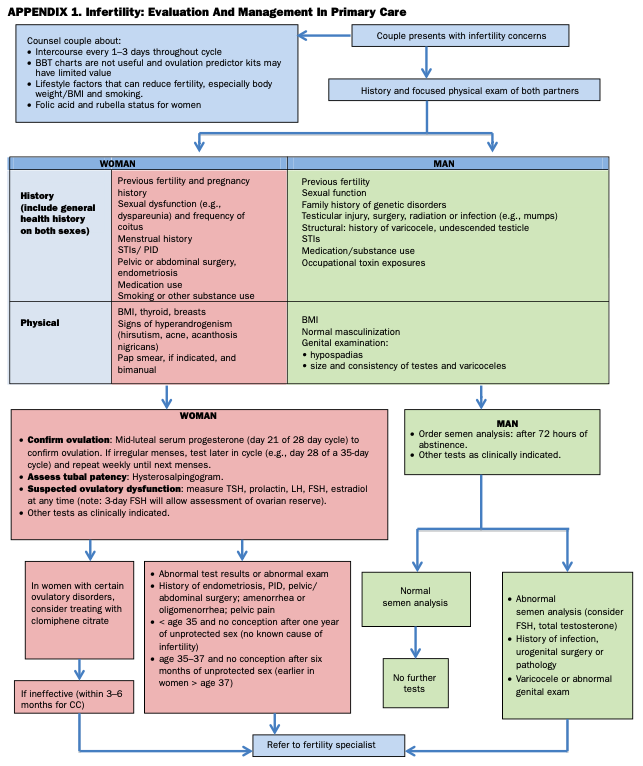
Before jumping into the history, a good phrase to have in your back pocket in family practice to potentially uncover younger couples who might be having trouble conceiving and didn’t think to bring it up is “what are your family plans?”. Regardless if that occurs, or if concerns with fertility are raised outright, some key things to ask about on history can be easily remembered by the mnemonic STOP, courtesy of Dr. Kotaska, which stands for Sex and Semen, Tubes, Ovulation and Pelvis:
- Firstly, get the patient’s GTPAL. Is this their first pregnancy or have they had prior? This will determine whether you’re potentially looking at primary or secondary infertility. Ask the partner where they have had children with previous partners too.
- Sex and Semen: when and how often are they having sex? Are they using lubricants? Are there any concerns regarding the semen?
- Tubes: do they have a history of STIs or PID that may compromise fallopian tube patency?
- Ovulation: what’s their cycle like, are they ovulating? Length and regularity? Regular menses every 24-35 days associated with premenstrual molimina (breast tenderness, bloating, cramping, and mood changes) is compatible with ovulation in at least 95% of women. A history of very irregular cycles suggests anovulation.
- Pelvis: do they have menstrual pain? Any signs of PCOS?
- How long they’ve been trying to get pregnant (this is a KEY QUESTION as this can determine whether or not you should start investigations for infertility)
- If the history suggests anovulation, evaluate for its various causes:
- screen for PCOS by asking about hirsutism, acne, alopecia, and weight gain.
- Hyperprolactinemia can present as headache, vision changes, galactorrhea or nipple discharge, although usually is asymptomatic aside from amenorrhea.
- thyroid dysfunction,
- premature ovarian failure (hot flashes and vaginal dryness), and
- hypothalamic dysfunction (eg eating disorder or excessive exercise).
- endometriosis will have dysmenorrhea, dyspareunia or dyschezia.
- History of pelvic infections or surgery or chemotherapy.
- Medication use, especially OCP (that would be an easy fix wouldn’t it! Gotta stop the birth control pill to try getting pregnant!). Assess whether they’re taking a PNV/folic acid.
- Family history of congenital or chromosomal abnormalities.
- Questions for the male partner include:
- screening for erectile dysfunction and
- genital injury or infections,
- or idiopathic causes such as tight underwear or pants, heat exposure or hot tubs, and marijuana use.
- Also do a quick screen for Klinefelter’s (tall, thin, gynecoid appearance) and visible androgen imbalances (gynecomastia, lack of body hair or hypospadias).
There is no objective for the physical exam here, but that doesn’t mean we’re not going to talk about it. It is almost always important to lay eyes/hands on the patient! For the female partner, get a height and weight to assess BMI. As usual, target your exam depending on your history: examine thyroid and breasts if concern was raised for thyroid dysfunction or galactorrhea.
Look for signs of hyperandrogenism as mentioned above: hirsutism, acne and acanthosis nigricans. A bimanual exam could be indicated if history is suspicious for endometriosis or pelvic adhesions, looking for a fixed, retroverted uterus, adnexal masses or tenderness, and uterosacral ligament thickening, nodules or tenderness.
If a pap smear is not up to date and you somehow have time in your busy day, you can do that plus swabs for STIs as needed.
For the male partner, you can do a genital exam to assess the testicles for varicoceles, testicular size, hernias or masses, however I don’t think this is commonly done at the onset of
workup unless the semen analysis comes back abnormal.
Back to the case: Shelley tells you they have been trying to conceive for 14 months and are having sex three times a week, without a condom (of course!). She gets her period every 6-8 weeks lasting for 1 week, and it has been that way for the last 6 years or so since she finished accounting school. Her periods aren’t painful or heavy, and she states there is no pain with intercourse. She has no other medical or surgical history and takes only a PNV.
Neither she nor her partner has had children with previous partners. Mike has no history of genital injury, infections or erectile dysfunction, and he says “I hate tight pants and underwear!”. Neither uses marijuana nor other drugs.
On exam, Shelley has a BMI of 36 with some facial hair visible around her jaw line and vermillion border as well as acne on her face and chest. Breast and pelvic exams are unremarkable.
When should you investigate infertility? That depends on the age of the female.
- If they are less than 35 years old, you should start a workup after 1 year of regular unprotected intercourse.
- If they are 35-40 years old, that time span shortens to 6 months.
- And if they’re over 40, investigate immediately as time is of the essence here.
Regardless of age, if there is a history of PID, infertility in previous relationships, prior pelvic surgery, chemotherapy/radiation in either partner, moderate-severe endometriosis, amenorrhea, or recurrent pregnancy loss, or the male has an abnormal semen analysis or other concerning findings, you should start investigating sooner than the above-mentioned time frames.
Objective Two

In these scenarios, you will inevitably get asked “what are the chances we can get pregnant?”. The general rates of couples achieving pregnancy are 75% within 6 months, 85% within 1 year, and 90% within 2 years.
The mean time to conception (ie the time at which 50% of women have conceived) increases with age from:
- 4 months in women younger than 30 to
- 9 months in women older than 35.
To look at it another way, for the 20-24 age group, 86% conceive within 1 year, whereas the 35-39 age group has a 52% 1 year conception rate, so 1 in 2 odds.
Success rates for natural fertility and assisted reproductive technology (except with egg donation) are significantly lower for women in their late 30s and 40s.
After hopefully not terrifying the couple with statistics if they lie on the unfavorable side, be sure to provide preconception counseling. Advise that delaying childbearing until the mid-30s may result in an increased frequency of pregnancy complications such as spontaneous abortions and chromosome abnormalities.
There is also an increased risk of perinatal mortality. Encourage optimization of health (especially aiming for a normal BMI, quitting/avoiding smoking/drugs/alcohol), and consider throwing an A1C on the prenatal lab req to screen for diabetes, alongside your office BP to assess for HTN. Regarding intercourse timing, optimal is every 2 days from 5 days before until 1 day after the predicted day of ovulation, with the most high yield window being between 48 hours prior to and up to 24 hours after ovulation. Ovulation predictor kits can help with this timing, provided the woman is not anovulatory. If the couple isn’t keen on tracking ovulation, keeping a regular frequency of intercourse every 2 or 3 days should be encouraged. Of course, all women considering pregnancy should take folic acid (0.4mg/day minimum) to reduce the chances of having babies with neural tube defects.
You will also inevitably be asked “why aren’t we able to get pregnant?”. While many couples may get pregnant in due time, 10-15% will be diagnosed with infertility, with causes divided into ⅓ female factors, ⅓ male factors, and ⅓ combined/unexplained factors.
However, with rising rates of obesity in increasingly younger women and a rise in obesity-related medical issues such as PCOS, we are seeing female factors account for more than the previously seen ⅓ of infertility causes. See the breakdown in the show notes for all the possible etiologies.
Objective Three

We went over this in objective 1: if someone is over >35, they should be worked up for and referred for infertility after 6 months of trying to conceive. If over 40, refer immediately.
Objective Four

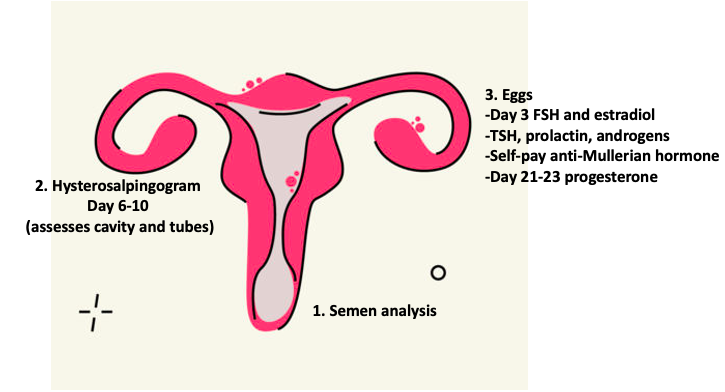
Investigations are tailored to the three ingredients of pregnancy:
1. Working sperm
2. Patent tubes and uterus
3. Working eggs
A basic workup includes a
- b-HCG,
- bloodwork for the female including a hormonal profile (Day 3 FSH, LH, prolactin, TSH, estradiol, as well as total testosterone if hirsute).
- You want FSH under 8-10.
- Upper limit of normal for testosterone is around 2.5 but above 1.5 can be considered hirsute.
- Don’t forget about the guy in your initial workup, as working sperm are one of the three pregnancy ingredients! Always get a semen analysis right off the bat.
Regarding the patent tubes and uterus, in my centre (Yellowknife, NWT), the OBGYN’s do not expect us to order a hysterosalpingogram (HSG) before referring to them, but please see what is done at your site. If there is concern for STIs, swabs can be done on one or both partners.
To confirm whether ovulation is taking place, a day 21 (luteal phase) serum progesterone is the gold standard. Keep in mind that the day 21 part is based on a 28-day cycle, however it should be done 7 days prior to the next menses, so if your cycle is 35 days, the progesterone should be checked on day 28 instead. Ovulation predictor kits nowadays sense the LH surge prior to ovulation, so are a less invasive method of assessing ovulation.
Further work-up your local OBGYN might undertake includes karyotyping, rubella and varicella serologies, a pelvic ultrasound to rule out a myoma or ovarian cyst, a hysteroscopy to visualize the uterine cavity, and an HSG as mentioned above, which can in fact be therapeutic and open blocked tubes. This test is ideally done on day 6-10 of the cycle, after the period but before ovulation.
For the male, the semen analysis should ideally be after 2-7 days of abstinence. This can be repeated in 3 months if the initial is abnormal (sperm have a 70 day life cycle).
Be sure to know your lab’s policies for semen analyses: they generally need to be kept warm (like under your arm warm), and brought to the lab within 30 minutes of collection to maintain viability for testing.
Normal parameters of a semen analysis are listed on the lab result; we won’t go through them today because there’s no need to remember them. Karyotyping and free testosterone can also be tested for the male if further workup is indicated.
For women over age 35 or anyone with risk factors for decreased ovarian reserve, testing of the ovarian reserve may be considered.
This is also known as the anti-mullerian hormone, or AMH, where the more ovarian follicles a woman has, the more anti-Müllerian hormone her ovaries can produce. The prompt for this test would be age of course, as well as a day 3 FSH greater than 10, signaling a decreased reserve.
A reassuring result is >1. This test is mainly used to predict the success of IVF. AMH levels peak around puberty and remain relatively constant until after menopause, when no follicles remain, and levels of AMH become low.
At 35, half of eggs are abnormal, at 40 2/3 are abnormal, in earlier 40’s, 90% are abnormal, so with less eggs it becomes that much harder to find the normal eggs for egg retrieval in IVF.
Back to Shelley and Mike: having decided to start an initial workup for infertility, you send off a bHCG and hormonal profile for Shelley, which comes back with an elevated testosterone as well as an LH:FSH ratio greater than 2:1, and a semen analysis (normal). With your suspicion being raised for PCOS in this case, you also ordered an A1C which comes back at 6.3%.
Objective Five

For some reason, the objectives don’t go into treatment other than adoption. Well, the time might be right if treatment options fail, so let’s go through those first. Depending on the underlying problem, options include education, medical, surgical and others. As usual, start with education and lifestyle modifications.
For Shelley’s case, we will discuss lifestyle management of PCOS in the next objective.
With suspected PCOS causing her anovulation, weight control is key. Even 5-10% of a person’s body weight has been associated with an improvement in metabolic status, a reduction in serum androgen concentrations, and resumption of ovulation in some studies. Have a discussion to suss out their current exercise habits and work together to find options to fit more physical activity into each week. Diet modifications such as limiting simple carbohydrates can also be encouraged.
If coitus frequency is not at optimal frequency, advise increasing that or timing it relative to ovulation (2 days prior to 1 day following presumed ovulation, every other day. Fun fact: the egg only lives for 24 hours, whereas the sperm persists for 72 hours, hence the timed intercourse time-frame.
If anovulation is the issue, ovulation induction with medications is the place to start. This can be done with letrozole, which is now the first line treatment over clomiphene citrate which has a higher risk of multiples. These medications stimulate ovulation. See the show notes for more specifics about them.
Other options I will gloss over here: donor sperm, if azoospermia or oligospermia are the issues; surgery for uterine abnormalities, lysis of adhesions or endometriosis; intrauterine implantation of sperm if needing to bypass the cervix. For blocked tubes, we already talked about an HSG to potentially open them up.
Assisted reproductive technology (IVF etc) is a common technique as well. IVF involves numerous steps: ovarian stimulation with medication, egg retrieval surgically, fertilization, culture, embryo transfer and embryo freezing. Main risks of treatment include ovarian hyperstimulation syndrome, where you start leaking fluid into the abdomen, and multiple gestations.
After all this, or throughout if the couple brings up the idea, consider discussing adoption, plus or minus gestational carrier and surrogacy. This is very different in different places, so difficult to summarize on a Canada-wide podcast. Please ask around to find out how the adoption process works at your site. In general, it takes at least a year to get on the adoption wait list, and in the north, the number of babies is small, so if this is of interest to the couple, advise them to get through the administrative hurdles and social work visits early to get on the list.
Objective Six

We’ve been touching on this throughout our case where Shelley (spoilers) has PCOS, or polycystic ovarian syndrome. This is why it is best to do the full hormonal profile at the initial workup, to assess for systemic diseases that could be affecting infertility such as thyroid abnormalities, a prolactinoma, or hypopituitarism.
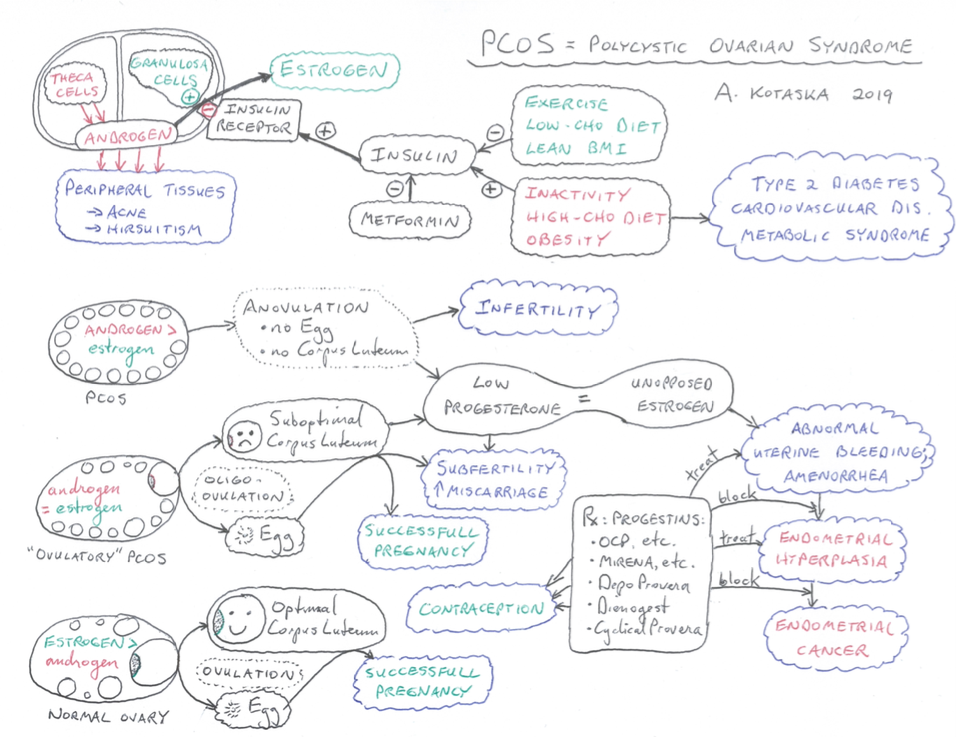
Let’s review how PCOS presents: it is caused by elevated androgen levels, so there is no LH surge to induce ovulation. We commonly see it in 15-35-year-old females. Symptoms include:
- anovulation, which can present as amenorrhea, oligomenorrhea, infertility or menorrhagia;
- obesity,
- insulin resistance, acanthosis nigricans;
- hirsutism and acne as manifestation of hyperandrogenism, and
- bilaterally enlarged polycystic ovaries.
There is often a family history.
Investigations will show:
- an elevated LH:FSH ratio greater than 2:1,
- increased DHEA (Dr. Kotaska never orders DHEA), and
- increased testosterone,
- and can also reveal polycystic ovaries on transvaginal ultrasound, although this is not required for diagnosis (need 2 of 3 of clinical or biochemical manifestations, anovulation and polycystic pathology on ultrasound).
- Fasting glucose may be elevated.
Treatment includes:
cycle control with
- weight loss,
- increased exercise,
- low carb diet,
- OCP (if not desiring pregnancy), and
- metformin.
Metformin should be trialed for roughly 6 months if PCOS is suspected, although current guidelines recommend against the routine use of metformin in obese women with PCOS, except in women with glucose intolerance who have failed lifestyle interventions.
Start low and go slow with metformin in this case, starting with 250 mg daily and gradually working your way up to 1g BID if tolerated. Continue the metformin until 12 weeks GA if pregnancy is achieved, as this can help combat higher miscarriage rates by maximizing the hormonal balance, and can also decrease in incidence of gestational diabetes if the patient doesn’t mind the medication and continues throughout pregnancy.
Menorrhagia.
TXA can be used for
Ovulation induction
is the next step with letrozole or clomiphene citrate.
Hirsutism
can be treated with OCP +/- spironolactone for antiandrogen effect, which is of course not compatible with pregnancy. Our reviewer Dr. Kotaska has drawn a fantastic PCOS schematic that you can check out in the show notes!
Hyperprolactinemia
generally presents simply with amenorrhea and a high prolactin level, but symptoms to watch out for include:
- galactorrhea,
- headaches and
- visual disturbances if a pituitary tumour is present.
Generally, imaging is normal if the tumour is micro, and even if it is macro (>10mm), they generally just need following, not surgical intervention. Treatment is with a dopamine agonist like bromocriptine or cabergoline which are safe in pregnancy.
Goal is to lower prolactin levels in order to resume ovulation and conceive. These medications act by inhibiting prolactin secretion and shrinking tumor size. If the prolactinoma is bigger than 10mm, it will need to be removed.
Hyperthyroid:
The thyroid will have its own podcast episode one day, but in this context, just be sure to recognize hyperthyroidism symptoms, which include anxiety, tremor, palpitation, wt loss, heat intolerance, increased appetite, and oligomenorrhea or amenorrhea.
Taking it back to Shelley and Mike for the last time to wrap up the case: with some fantastic lifestyle modifications and metformin, Shelley was able to bring her BMI down to 29. Using ovulation predictor kits, Shelley was able to confirm that she was ovulating, and 8 months later, her and Mike happily announced to you that they are 12 weeks pregnant and would like to talk about prenatal care.
A few take home points as we wrap things up for this episode:
•Think of the ingredients of pregnancy – working sperm, working eggs, and open tubes/uterus.
•Remember the different potential diagnoses
•As a family doc, if you’re thinking about referring, make sure you do a basic workup first: history, physical, semen analysis for the male, and a b-HCG and hormonal workup for the female
•Have a sense of the treatment options available
•Be sure to normalize infertility for the patient/couple!
•On the ethics side of things… Infertility demands non-judgmental discussion – refer if you’re not comfortable with prescribing the treatment options!
Resources Used
•Toronto Notes 2020
•UpToDate
•Workup for Infertility lecture by Dr. Hitkari
•My notes from teachings by Dr. Dobson (OBGYN in Trail)
•HIPPO Primary Care RAP Infertility – super helpful short podcast
•https://ccfpprep.com/category/fm-99-priority-topics/52-infertility/•PBSG https://members.fmpe.org/member/my_modules?overwrite_close=true&tab=available