
- Written By: Darrell Vandenbrink – FM PGY1 at Queens University
- Peer Review By: Chris Cochrane, and
- Expert Review By: Dr Adrienne Stedford – PGY3 in Calgary, Alberta
When assessing the acutely ill patient, look for signs and symptoms of dehydration. (e.g., look for dehydration in the patient with a debilitating pneumonia).
- For this objective, it is important to first be aware of general risk factors for all types of dehydration or hypovolemia. These include:
- Any acute illness, but especially if there is fever, vomiting or diarrhea
- Decreased cognitive function
- Reduced oral intake, which can occur for many reasons but some causes to consider are critical illness, dysphagia, need for assistance with feeding, and limited access to food or water because of poor mobility
- Absence or alteration thirst mechanism, which can be secondary to hypothalamic lesions or simply due to aging
- So be on the lookout for dehydration and hypovolemia in elderly patients who may suffer from delirium, dementia, dysphagia and a host of other conditions that put them at risk for fluid losses and poor oral intake.
- Next let’s review some common causes of the different types of dehydration and hypovolemia.
- Hypernatremic hypovolemia
- This is due to dehydration, which means loss of hypotonic fluids
- This can happen secondary to vomiting, diarrhea, fever, limited oral fluid intake, diuretics, skin losses such as burns or sweating, hyperglycemia causing osmotic diuresis as in DKA or HHS, and diabetes insipidus (either central or nephrogenic).
- If any of these conditions are present, and the patient has limited access to water or has impaired thirst mechanisms, they could become hypernatremic.
- Hyponatremic hypovolemia
- A lot of these causes are the same as those for hypernatremic hypovolemia. But in this case, Harrison’s Internal Medicine breaks down the etiologies into renal and extrarenal causes.
- Renal causes include diuretics, osmotic diuresis from DKA or HHS, adrenal insufficiency, salt wasting nephropathy and cerebral salt wasting. Note that diuretics and osmotic diuresis can cause either hypernatremic hypovolemia or hyponatremic hypovolemia
- Extrarenal causes include GI losses from diarrhea or vomiting, skin losses such as sweating or burns, and third spacing from conditions like sepsis and pancreatitis.
- A lot of these causes are the same as those for hypernatremic hypovolemia. But in this case, Harrison’s Internal Medicine breaks down the etiologies into renal and extrarenal causes.
- Isotonic hypovolemia
- May occur from bleeds, extreme GI losses from vomiting or diarrhea, and trauma.
- Hypernatremic hypovolemia
- When your patient has any of these conditions, you should assess for symptoms and signs of dehydration and hypovolemia. These are pretty nonspecific but include:
- Symptoms of…
- Fatigue, weakness, malaise, thirst and postural dizziness
- In more severe forms, you may see oliguria, confusion, obtundation and even cyanosis and abdominal or chest pain
- In pediatrics, symptoms might also include fewer wet diapers, irritability, and, if there is severe dehydration, lethargy or loss of consciousness.
- Signs on physical exam include…
- Diminished skin turgor, dry oral mucous membranes, decreased JVP, orthostatic tachycardia (defined as an increase in heart rate by 30bpm upon standing) or orthostatic hypotension (defined a drop in systolic BP of greater than 20 or drop in diastolic BP greater than 10)
- In extreme forms, the patient may go into hypovolemic shock, which would manifest as hypotension, tachycardia, peripheral vasoconstriction and hypoperfusion, oliguria and altered mental status
- In infants, also look for sunken fontanelles and absence of tears.
- Symptoms of…
- If this is all hard to remember, there is a mnemonic that a group called the Dehydration Council suggests using as a screening tool for dehydration risk. The mnemonic is DEHYDRATIONS
- D – diuretics
- E – end of life
- H – high fever
- Y – yellow urine turns dark
- D – dizziness, as in orthostasis
- R – reduced oral intake
- A – axilla dry – McGee gives this a LR of 3.0
- T – tachycardia
- I – incontinence
- O – oral problems
- N – neurologic impairment
- S – sunken eyes – LR of 3.7
- And McGee also includes:
- Dry mucous membranes with LR of 3.1, and
- Abnormal skin turgor with an LR of 3.5
In the dehydrated patient, assess the degree of dehydration using reliable indicators (e.g., vital signs) as some patients’ hydration status may be more difficult to assess (e.g., elderly, very young, pregnant).
- Volume status is difficult to assess, particularly in certain patient populations. For example, elderly patients may already have postural hypotension because of underlying diseases or they may have a dry tongue and mouth from their medications, not from dehydration. So we need to use a variety of reliable objective indicators to determine a patient’s volume status.
- There is a JAMA Rational Clinical Exam article titled “Is This Patient Hypovolemic?” which describes some of the most reliable clinical exam features for hypovolemia. The most reliable findings actually differ depending on if you suspect the patient is hypovolemic from blood loss or from vomiting, diarrhea or decreased oral intake.
- For patients with suspected blood loss
- The most helpful physical findings are either severe postural dizziness or a postural pulse increase of 30 beats per minute or more. These findings have a sensitivity of 97% for large blood loss and a specificity of 98%. By contrast, tachycardia or hypotension while supine are often absent with a sensitivity of only 33%. So this means that your patient could have lost a large volume of blood but still have a normal heart rate and blood pressure while supine and then you do postural vitals and you see the abnormalities – so get your orthostatic vitals!
- For patients with suspected blood loss
- For patients with vomiting, diarrhea or decreased oral intake:
- Dry axilla has a positive likelihood ratio for hypovolemia of 2.8
- Moist mucous membranes and a tongue without furrows argue against a diagnosis of hypovolemia, with a negative likelihood ratio of 0.3
- Even though we often look for them, cap refill and skin turgor weren’t found to have diagnostic value in this article.
- Beyond these physical exam findings, we can use investigations as well. Although they are also non specific, things we can look for include:
- Urine output: less than 0.5 ml/kg/h suggests volume depletion
- Bloodwork may show abnormalities including
- BUN and creatinine may be elevated
- Hematocrit may also be high
- Electrolyte abnormalities
- Acid base disturbances
- Elevations in liver enzymes or troponins if hypovolemia is severe enough to cause ischemia
- Urine sodium concentration: this is actually one of the most reliable ways to diagnose hypovolemia, which will typically be low if there is hypovolemia because the kidneys retain sodium and water to try to maintain intravascular volume
- POCUS for IVC assessment
- If you are adept at POCUS, this is a great way to assess volume status – you look at the IVC and determine its size and collapsibility with inspiration. If the IVC diameter is <1cm and obviously collapses with inspiration, the patient is more likely hypovolemic and will respond to fluids.
- If you are adept at POCUS, this is a great way to assess volume status – you look at the IVC and determine its size and collapsibility with inspiration. If the IVC diameter is <1cm and obviously collapses with inspiration, the patient is more likely hypovolemic and will respond to fluids.
- Pediatrics
- In pediatrics, it is actually easier to quantify the degree of dehydration. If you have a baseline weight, you can just calculate the percent weight loss to determine the degree to dehydration. UpToDate has a nice table summarizing findings for mild, moderate and severe dehydration that we will include in the show notes.
- Mild – 3-5% weight loss
- In this category, there are symptoms of dehydration based on history such as increased thirst and slightly reduced urine output as per parents
- Moderate – 6-9% weight loss
- There are physical exam findings of dehydration such as tachycardia, dry mucous membranes, sunken eyes and fontanelles and reduced skin turgor
- Severe – >9% weight loss
- Mild – 3-5% weight loss
- In pediatrics, it is actually easier to quantify the degree of dehydration. If you have a baseline weight, you can just calculate the percent weight loss to determine the degree to dehydration. UpToDate has a nice table summarizing findings for mild, moderate and severe dehydration that we will include in the show notes.
- There are signs shock such as low blood pressure, mottling and lethargy or coma

In a dehydrated patient,
Determine the appropriate volume of fluid for replacement of deficiency and ongoing needs
Use the appropriate route (oral if the patient is able; IV when necessary).
- The nuances of fluid management is a very big topic, so we will just provide an overview here.
- So obviously, if the patient has electrolyte abnormalities like hypo or hypernatremia or if they are hypovolemic from bleeding, you will need to treat those very differently. Of course, with bleeding you’re going to replace losses with blood products, but that’s a discussion for another episode. Here, we will focus on treatment of hypovolemia without electrolyte abnormalities and without bleeding.
- The main treatments will be oral rehydration therapy and IV fluids.
- Oral rehydration therapy is the best option for dehydration in both kids and adults if the patient can tolerate it and the dehydration isn’t severe, so there isn’t the need for rapid rehydration. In children, we often use Pedialyte for this.
- IV fluids
- If the patient can’t tolerate PO fluids despite appropriate treatment with antiemetics or if they have severe dehydration, you need IV fluids or even IO if you can’t get IV access
- If the patient is hemodynamically unstable with abnormal vital signs, start with bolus doses of crystalloid – this is typically 1 or 2 20ml/kg boluses in children and 1 or 2 500cc-1L boluses in adults although the rate should be tailored to the clinical scenario.
- Once the patient is stable, if they aren’t drinking or eating well yet, you need to start maintenance fluids. In kids, you can calculate the maintenance rate using the 4:2:1 rule – 4ml/kg/h for the first 10kg of the child’s weight, 2ml/kg/h for the 2nd 10kg and 1ml/kg/h for each kg above 20kg. We will have a worked example in the show notes.
- Worked example:
What is the maintenance IV fluid rate for a 12 year old girl who weighs 42kg?- 4:2:1 rule (4ml/kg/h for the first 10kg of the child’s weight, 2ml/kg/h for the 2nd 10kg and 1ml/kg/h for each kg above 20kg)
- So, for a patient who weighs 42kg, this becomes:
- 4ml/kg/h x 10kg = 40ml/h for the first 10kg
- 2ml/kg/h x 10kg = 20ml/h for the next 10kg
- 1ml/kg/h x 22kg = 22ml/h for the last 22kg
- Total = 40+20+22ml/h = 82ml/h
- So, for a patient who weighs 42kg, this becomes:
- 4:2:1 rule (4ml/kg/h for the first 10kg of the child’s weight, 2ml/kg/h for the 2nd 10kg and 1ml/kg/h for each kg above 20kg)
- Worked example:
- For peds this maintenance fluids should be IV crystalloid – Tintinalli’s suggests 0.9% normal saline with 5% dextrose and UpToDate recommends adding 10-20mEq of KCl to each litre of fluids to avoid hypokalemia
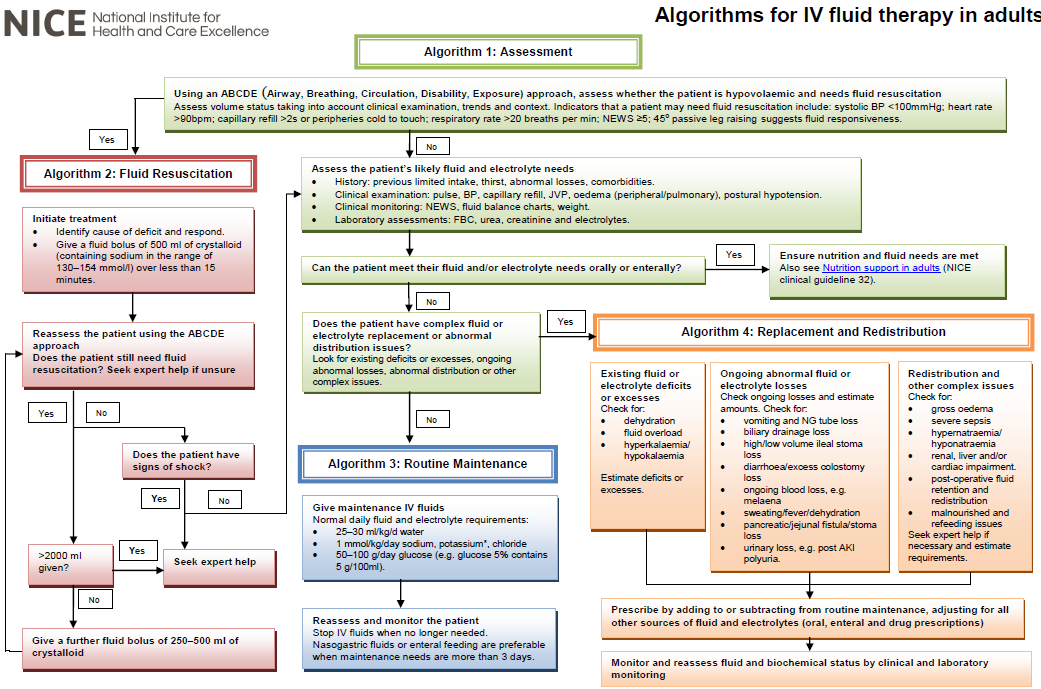
In adults, we were only able to find one guideline that (A) gave recommendations for how to accurately calculate the appropriate volume of maintenance fluid for adults and (B) wasn’t for a specific population like sepsis patients or people with AKI in the ICU. This is a guideline for Intravenous Fluid Therapy in Adults in Hospital out of the UK from the National Institute of Health and Care Excellence, which is also called “NICE”.
However, the recommendations in this NICE guideline are pretty complicated and, in our estimation, of questionable utility in clinical settings. They recommend that maintenance fluids should be 25-30ml/kg/d of water, 1mmol/kg/d of sodium and potassium and 50-100g/d of glucose. For a 70kg person, this would work out to about 75cc/hr of D5 and ½ normal saline with 3 doses per day of 20mEq of KCl. This is pretty complicated to work out for every patient you have on IV fluids, which is probably why we typically see clinicians just choosing a fluid and rate that seems reasonable based on their clinical judgement.
- This is more of the approach that UpToDate takes – they simply state that, to account for a patient’s needs for water, electrolytes and glucose, it reasonable to start with 2 liters per day, which is about 80cc’s per hour, of half normal saline in 5% dextrose with 20mEq of potassium chloride added to each liter of fluid. And remember, you also need to consider what ongoing fluid losses the patient has and increase the volume of IV fluids as necessary to account for those ongoing losses.
- For anyone who is interested, the NICE guideline does have a pretty nice algorithm for choosing IV fluid therapies for your patients that we will have in the shownotes.
When treating severe dehydration, use objective measures (e.g., lab values) to direct ongoing management.
This objective emphasizes the importance of reassessing your patient when you are treating severe dehydration. This should include clinical assessments of volume status as well as ongoing monitoring of urine output, lab values and maybe POCUS for IVC collapsibility. If you want, you can also track daily weights. In terms of lab values, signs of resolving dehydration would include normalization of BUN and creatinine, as well as lowering of hematocrit. If your patient had electrolyte abnormalities to begin with, you should also monitor those regularly to ensure they normalize with treatment.
In a dehydrated patient
Identify the precipitating illness or cause, especially looking for non-gastro-intestinal, including drug-related, causes
Treat the precipitating illness concurrently.
- So this objective is pretty self explanatory and harkens back to objective 1 where we listed various etiologies of dehydration and hypovolemia. It’s important to consider not only the dehydration itself but the underlying cause. Let’s quickly review some common examples:
- If a medication is contributing to the dehydration, stop or reduce doses of offending agents such as diuretics.
- If there is hyperglycemia causing osmotic diuresis, treat with fluids and insulin per your DKA/HHS pathway.
- If there is an infection causing fluid losses secondary to fever, treat the underlying infection with appropriate antibiotics and use antipyretics to bring down the fever.
- If there are significant losses from emesis, treat with antiemetics, and identify the underlying cause for the vomiting, be that infectious causes, GI related disorders affecting the pancreas or biliary system, or even CNS causes.
- Once the underlying cause is addressed, the fluid losses should lessen and hopefully the patient will feel well enough to maintain their own fluid balance by eating and drinking on their own.
Treat the dehydrated pregnant patient aggressively, as there are additional risks of dehydration in pregnancy.
- Pregnant patients have higher water intake requirements than people who aren’t pregnant and they can get pregnancy-specific conditions like hyperemesis gravidarum that put them at particular risk of dehydration and hypovolemia.
- Also, if a pregnant patient does become dehydrated, there are greater risks involved. Although the evidence isn’t of great quality, dehydration has been associated with:
- Gestational hypertension and preeclampsia
- Gestational diabetes
- Preterm birth
- Oligohydramnios
- Low fetal birth weight
- So it’s really important to counsel pregnant patients on adequate fluid intake and to assess volume status in pregnant patients who are unwell. If you suspect your pregnant patient is dehydrated, treat aggressively with oral rehydration or IV fluids to prevent the complications of dehydration and hypovolemia.
Resources Used
- Associations between hydration state and pregnancy complications, maternal-infant outcomes: protocol of a prospective observational cohort study. https://pubmed.ncbi.nlm.nih.gov/32033597/.
- DynaMed. Dehydration and hypovolemia in adults. https://www.dynamed.com/condition/dehydration-and-hypovolemia-in-adults.
- Harrison’s Principles of Internal Medicine, 20th Edition.
- Inferior vena cava collapsibility detects fluid responsiveness among spontaneously breathing critically-ill patients. https://pubmed.ncbi.nlm.nih.gov/28525778/.
- POCUS Cases 7 IVC for Volume Assessment. https://emergencymedicinecases.com/videos/pocus-cases/.
- The rational clinical examination. Is this patient hypovolemic? https://pubmed.ncbi.nlm.nih.gov/10086438/.
- Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8th edition.
- UpToDate. Clinical assessment and diagnosis of hypovolemia (dehydration) in children. https://www.uptodate.com/contents/clinical-assessment-and-diagnosis-of-hypovolemia-dehydration-in-children?search=hypovolemia&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=3.
- UpToDate. Etiology, clinical manifestations and diagnosis of volume depletion in adults. https://www.uptodate.com/contents/etiology-clinical-manifestations-and-diagnosis-of-volume-depletion-in-adults?search=hypovolemia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
- UpToDate. Etiology and evaluation of hypernatremia in adults. https://www.uptodate.com/contents/etiology-and-evaluation-of-hypernatremia-in-adults?search=evaluation%20of%20hypernatremia&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
- UpToDate. Maintenance and fluid therapy in adults. https://www.uptodate.com/contents/maintenance-and-replacement-fluid-therapy-in-adults?search=maintenance%20fluids&source=search_result&selectedTitle=3~150&usage_type=default&display_rank=3#H5.
Williams Obstetrics, 25th edition.

One thought on “CCFP Topic: Dehydration”