
- Written/Researched By: Braedon Paul
- Peer Review By: Caleb Dusdal
Step One
For this one, active and reflective listening without inserting your opinion is key. As always, ask open-ended questions, use encouraging statements, and throw in some of those nonverbal communication techniques (eg, seated and leaning forward, making eye contact, nodding along).
If they are distressed, encourage deep breathing or mindfulness techniques. Commend the patient for coming and validate their experience, which importantly does not require you to necessarily agree with their view or response to this crisis.
Also important in this step is to avoid triggering any re-traumatization through your words or actions. This is something that sounds obvious but even seemingly innocuous comments or references to the trauma can be traumatizing to patients, particularly those at risk of acute stress disorder or post-traumatic stress disorder.
In general, let the patient themselves establish the boundaries of conversation and avoid prodding around sensitive topics unnecessarily. When possible, explain the rationale behind the sensitive questions you might ask.
The key to step 1 is this: You are the proverbial shoulder to cry on. Reassure them that they’re in a safe space and that you are there to listen without judgement.
Step Two
Remember, the more information you have the better. Aside from the subjective information gleaned during your interview, don’t forget about that objective component as they sit in front of you – how do they look, how are they behaving, what’s their insight like? How worried are you that they intend to harm themselves or someone else?
For this part, ask them directly if they have suicidal or homicidal thoughts or intentions. That said, keep in mind that some patients may be in a mental or psychiatric state that limits the reliability of their information.
In these scenarios, you might have to contact a family member or close friend for more information, particularly if you have any concern whatsoever about their safety and well being.
Step Three
So, step 3 builds off step 2, which was about establishing severity. Now its all about safety: the patient’s safety, your own safety, and the safety of any other parties who might be implicated or affected.
Keep in mind that physicians do have a duty to warn and protect intended victims of a patient, if you are reasonably convinced that they are at risk of imminent harm.
If, alternatively, it is the patient themselves who is at immediate or serious risk from someone else (such as could be the case with intimate partner violence) they should be encouraged to remove themselves from the situation immediately to a shelter or other safe place, if possible. Taking a step back, encourage your patients who are less acutely at risk of harm to have an organized safety plan that can be acted on quickly if needed.
To ensure that you and your colleagues are safe, make sure to have procedures and policies for handling agitated or dangerous patients, which would typically include some basic training for all personnel. This will look different if you’re in a clinic, the wards, or the ER.
Step Four
You should ask about the patient’s use of inappropriate coping mechanisms such as denial, withdrawal, and reliance on harmful behaviors or use of substances – whether it be drugs or alcohol.
Address these as they arise, specific management is beyond the scope of this topic and will be highly case-specific – as you might expect.
For all patients, help them focus on their strengths and how these and other coping mechanisms were used successfully in the past. Along with their “internal” strength, encourage your patients to identify family, friends, and other external support networks.
Now’s also a great time to empower the patient with resources they can use on their own time, whether that includes online or printed self-help resources, mobile phone apps, or local counselors in the community. They may already have some that they’ve used in the past.
Another point to be aware of is that a subset of these patients may go on to develop depression, anxiety, an acute stress disorder, or even PTSD, and may therefore benefit from trauma-focused cognitive behavioural therapy, which is a form of CBT that is usually started within 2-weeks of a traumatic event and typically includes patient education, cognitive restructuring, and exposure therapy in order to reduce the severity of acute stress disorder symptoms and to prevent the development of PTSD.
Others may benefit from pharmacologic therapy, such as SSRIs, other antidepressants, or even anti-psychotics in some cases – which we won’t dig into on today’s episode, but you can check out our episode on Anxiety for more details on that.We will, however, take a brief moment to emphasize that benzodiazepines, although very effective when used responsibly, should be considered with a high degree of caution and only for those with intense anxiety, agitation, or sleep disturbance in the immediate period following a traumatic event, and for no more than 2-4 weeks given the potential for detrimental risks associated with long-term BZD therapy. That said, they can be an important tool in your toolbox and shouldn’t be shunned entirely – just make sure to co-prescribe with a large dose of patient education.
Step Five
At this point, you’ll be wrapping up your patient encounter, but its important to remember that, for the patient, the journey does not end here. Supportive follow-up is recommended to check on their status and to reinforce their positive efforts.
In doing so, you provide patients with a lifeline and improve the likelihood that they will follow through with the action plan.
An important item to keep in mind is not to cross boundaries when your patient is in crisis. This can be difficult because you are probably a bit of a bleeding heart, otherwise why are you a family medicine specialist?, and you just want to help them. But you have to remember to avoid making appointments with them outside normal hours or outside clinical spaces, and never to lend money or similar things.
As a quick reminder on action plans, remember that they should be SMART, that is, specific, measurable, attainable, relevant, and time-based. Check out our Counselling episode for more details, which also includes a fantastic section on some motivational interviewing techniques – so we won’t cover that here.
The PorticoNetwork, which we have referenced before, is a Canadian source for mental health education from a Primary Care perspective. Similar to the management plans we use for Asthma and COPD in collaboration with the patient, they have a Crisis Prevention and Management Plan. We will link to this document in the Show Notes. It is essentially a formalization of signals that the patient can notice to trigger the need to intervene, and then a planned intervention depending on the stage of crisis that is being experienced.
Of course these signals and interventions are collaborated on with the patient, their caregiver and yourself to ensure buy-in from everyone and to find a solution that fits their context best. The plan we have linked to is for patients with developmental disabilities who might be more prone to having crises, but the principles are widely applicable.
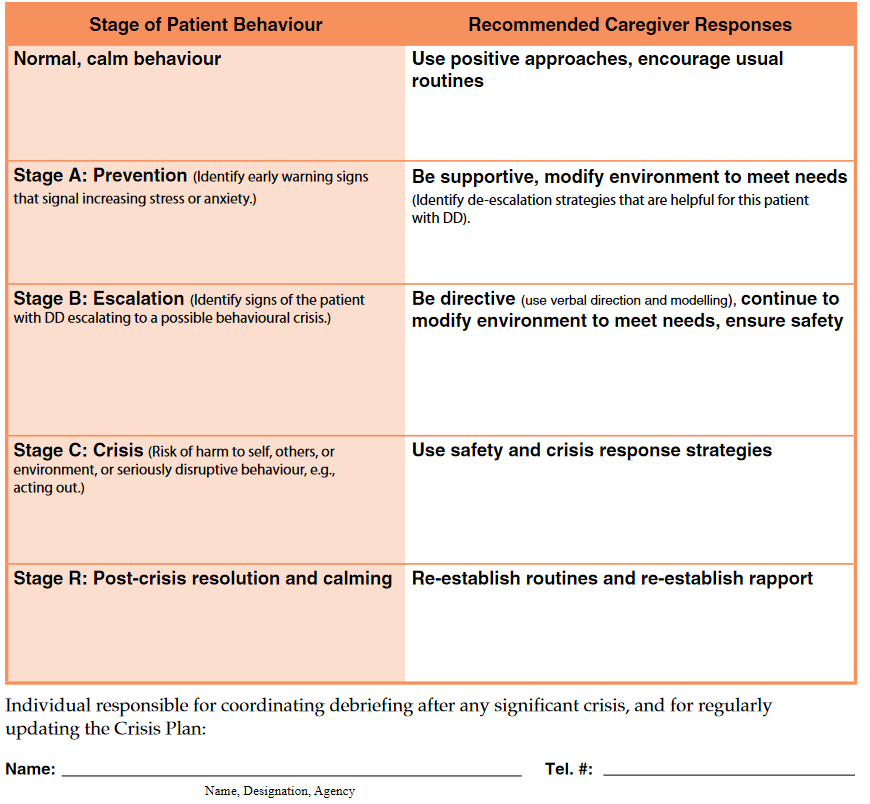
The PorticoNetwork has taken some Holistic Crisis Planning tools that were developed in Ohio, and through the Peel Service Collaborative in Ontario, adapted them to the Canadian Primary Care context. They have an outline of the approach based on guidelines as well, which we will link to for you, into ten general steps. We won’t cover them here, but recommend them for your practice.
During follow-up, assess their progress regarding the specific plan of action and reinforce even small therapeutic gains. If appropriate, try and have the patient reflect on potentially positive outcomes related to the crisis whether it be improved self-discipline, a feeling of competence, or a sense of future ability to cope with adversity.
For some patients, this follow-up with you as their family doctor could be sufficient. That said, have a low threshold for involving other professionals and support services in patients who you think might require a higher and more intense level of care – especially if you suspect acute stress disorder, which can of course further progress into PTSD if left unaddressed.
As a side note, psychological debriefing (also known as “critical incident stress debriefing”) has not been found to be effective in preventing PTSD among individuals experiencing a traumatic event, and while trauma-focused CBT is ideally delivered within 2 weeks of the traumatic event – some patients, such as the acutely grieving or suicidal, might benefit from a further delay to therapy so that more urgent problems can be addressed.
The gist of it is this: Ask for help when you need it. You’re not an island, and the truth is that you often won’t have the people, resources, or time necessary to tackle these cases on your own. Keep a list of services of this kind that are available in your local community so you can pull it out if and when you need it.
And with that, we wrap up the five steps. It might seem like a lot, but it really boils down to a few core principles.
Case Resolution
Mary joins you in your office and appears to be visibly emotional.
“I just lost my job because of the COVID. I worked there for several years. I’ve got two young children and that was our source of income. These past two days have been terrible, I can’t stop crying. what will our family’s future look like? I’m having trouble concentrating, I can’t sleep and or eat.“
You offer her a tissue and give her some time to explain her recent struggles to you in more detail. As she speaks, you maintain eye contact, nod along at times, and acknowledge the challenge of her experiences without inserting any of your own judgements or opinions.
You use open-ended questions to glean more information and make a point to ask about coping mechanisms – particularly harmful ones such as an increased use of alcohol or drugs, all of which Mary denies.
You also take this time to run through a quick mental status exam. Mary is a middle-aged and well-kept woman who appears her stated age. She appears quite emotional, with limited eye contact and a somewhat hunched posture. She is an accessible and reliable historian with a logical thought form and content. Her speech is quiet but otherwise normal. She describes her mood as “crushed” and her affect appears to be moderately dysthymic.
Insight and judgement were intact, and there was no evidence of any perceptual or cognitive abnormalities.
When asked directly, she does not endorse homicidal ideation and, when asked about suicidal ideation, she states:
“Since I lost my job, I’ve found myself sometimes thinking it would be better if I never woke up – but I’ve never wanted to act on anything like that”.
When questioned further about this, she’s able to identify a strong support network among her partner and a few close friends and emphasizes that she feels comfortable reaching out to these people when she gets overwhelmed.
You acknowledge her courage in disclosing this information to you and provide her with the contact details for a local counselor in the community. You additionally provide some recommendations for online self-help resources, such as the freely available anxietycanada.com, which contains a number of self-guided tools designed to help patients navigate their mental health.
You also briefly discuss medication options with Mary, but you both agree that starting with a trial of non-pharmacologic options is more ideal in her case – particularly as you can find no evidence of any severe or disabling symptoms at this time.
As you have identified no safety concerns, you get ready to wrap up Mary’s appointment, having armed her with an action plan and self-help resources, contact details for the local counselor, and a follow-up appointment in your clinic in 2 weeks time.
While you have educated Mary about the importance of reaching out to friends, family members, or professional help hotlines or emergency services should her mental state take a turn for the worse, you’re careful not to cross any professional boundaries by providing your personal contact details or agreeing to meet outside of regular clinic hours.
Two weeks later, she returns to your office, and appears to be in much better spirits.
“I checked out the online resources you gave me and also had one session with a counselor, and we got along pretty well, so I plan on continuing to see her. I am still without a job and have stress related to this, but I feel like I am at least now in a mental space where I feel capable of getting back in the job market. I also applied for the government’s COVID recovery benefit.”
She thanks you for your support, and you pat yourself on the back for another job well done.
And, with that, we bring the case to a close
Resources Used
- A Practical Guide to Crisis Management, AAFP 2006
- Providing Trauma-Informed Care, AAFP 2017
- Treatment of acute stress disorder in adults – UpToDate
- Portico Network – Holistic Crisis Planning Toolkit https://www.porticonetwork.ca/tools/toolkits/hcp-toolkit
- Portico Network – Crisis Prevention and Management Plan https://www.porticonetwork.ca/documents/38160/869447/ED_Crisis+Prevention+and+Management_APP.pdf/262207e3-130c-4bc6-a630-2ba10c679d09
