
- Written By: Caleb Dusdal
- Peer Review By: Sarah Donnelly
- Episode Art and Infographic By: Aikansha Chawla
Objective One:
In patients complaining of leg pain and/or swelling, evaluate the likelihood of deep venous thrombosis (DVT) as investigation and treatment should differ according to the risk.
Only about 10% of suspected cases end up being a DVT, that’s a lot of resources for so many negatives. Thus why its so important to establish an accurate pre-test probability beforehand.
The ubiquitous Wells DVT score is probably the most familiar validated tool. You probably also know there is both a three tier form, breaking results into: low, moderate and high likelihood, as well as a two-tier which just separates it into ‘unlikely’ and ‘likely’.
Thrombosis Canada 2020 VTE Guidelines only list the easier two-tier version, and so that is what we are focusing on here.
A Wells score of 0 points or one point equates to ‘unlikely’ and suggests 6% risk of a DVT being present.
2 or more points equates to ‘likely’ and was validated as a 28% chance of having a DVT.
Of course there is also a clinical gestalt scoring item in the rule. If you think another diagnosis is more or just as likely, then subtract 2 points from the score.
There are nine items making up the Wells score, each one adding 1 point to the score if present. The table of each item is in the show-notes for your review, and we’ll cover them quickly now as the first step of your spaced repetition:

The benefit of going through the process of getting your patient’s Wells score is that your patient now falls into either unlikely or likely category and this can be helpful to guide whether or not you move forward with more investigations.
Lets summarize the diagnostic approach to DVT, as it can be a bit difficult to follow:
- First, do a history and physical looking for the 9 items on the Wells Score
- An ‘unlikely’ pre-test probability(score of 0 or 1) should have d-dimer done
- If d-dimer is positive, you probably need to get compressive ultrasound study done
- If d-dimer is negative, you’re in the clear and need to pay more attention to other items on your differential
- If you score a ‘likely’ pre-test probability(2 or more) then go ahead and go straight to compressive ultrasounds study
- If compressive ultrasound study is negative, but you still think DVT is the most likely cause for their symptoms
- Get a d-dimer
- If negative, then don’t worry about it
- Get a d-dimer
- If compressive ultrasound study is negative, but you still think DVT is the most likely cause for their symptoms
- An ‘unlikely’ pre-test probability(score of 0 or 1) should have d-dimer done

Objective Two:
In patients with high probability for thrombotic disease (e.g., extensive leg clot, suspected pulmonary embolism) start anticoagulant therapy if tests will be delayed.
Thrombosis Canada agrees with this. They say that unless compression ultrasound study is available right away, the number they give is within 4 hours, you should start anticoagulation for moderate to high likelihood(if using three-tier rule) or ‘likely’ using the simplified two-tier, of having a DVT.
You should also use something that will provide immediate effect, so not Warfarin on its own. This means, a DOAC, or LMWH bridging to Warfarin.
I don’t know about you, but the convenience of a DOAC seems the way to go these days, and they have also shown to be just as effective as Warfarin with lesser bleed risk.
The exception is if your patient, for whatever reason, does not have coverage. DOACs are pricey while Warfarin is cheap like borscht.
Objective Three:
Identify patients likely to benefit from DVT prophylaxis.
Thrombosis Canada’s guidelines divide these patients into:
– Hospitalized Medical Patients
– Non-orthopaedic Surgery Patients
– Orthopaedic Surgery Patients
– Superficial Venous Thrombosis or Thrombophlebitis
Hospitalized Medical Patients
Risk factors for VTE in medically ill inpatients include:
– Age over 70 years
– Previous VTE
– Immobility for 3 or more days
– Stroke
– Acute spinal cord injury
– Active cancer
– Known thrombophilia (could build on this if not elsewhere in the episode?)
– Sepsis
– Acute inflammatory conditions (examples?)
– Acute infectious disease
– Obesity, which is a bmi > 30
– Hormone therapy
– ICU admission
– Respiratory or Cardiac failure
This, of course, needs to be balanced against their risk of bleeding, otherwise they may not benefit overall from anticoagulation. Some of the risks for develop bleeding are:
– Active gastroduodenal ulcer
– Previous bleed in the past 3 months
– Advanced age (ironic given we just said advanced age is risk for clots)
– Severe renal failure (<30 mL/min)
– Hepatic failure, which is in question actually because your liver produced both pro and anti coagulant enzymes, so their actual bleed risk is unknown despite prolonged INR (INR only measures the procoag function)
– Active cancer
– Platelet count under 50 x 10^9/L
To balance these risks you can consider using the tool we mentioned before, the sparctool, though I believe this is intended for the outpatient.
Non-orthopaedic Surgical Patients
For most elective non-orthopaedic surgical patients, for whom thromboprophylaxis is indicated, and average bleed risk, consider starting prophylaxis within 12 hours of completion of the surgery.
If moderate to high VTE risk, thromboprophylaxis should be continued at least until discharge from hospital.
Could use up to 30 days after discharge in select populations.
The policy will likely vary by institution, but Thrombosis Canada via the American Society of Haematology(ASH) from 2019, does provide a table of recommendations depending on the type of non-orthopaedic surgery, which will be in the show notes:
Table 1: Surgical site-specific recommendations:
| Patient group | ASH guideline panel recommendation | Notes |
| General surgery | Suggests pharmacological thromboprophylaxis* | · May not apply to patients undergoing laparoscopic cholecystectomy· Consider extended duration thromboprophylaxis (e.g. up to 30 days) for high risk cancer surgery |
| Neurosurgical | Suggests against pharmacological thromboprophylaxis** | · May not apply to patients at higher risk for VTE |
| Transurethral resection of the prostate orRadical prostatectomy | Suggests against pharmacological thromboprophylaxis** | · May not apply to other urological procedures and/or in patients at higher risk for VTE |
| Trauma | Suggests pharmacological thromboprophylaxis if low risk of bleeding*Suggests against pharmacological thromboprophylaxis if high risk of bleeding** | · Consider extended duration thromboprophylaxis (e.g. until discharge from rehab centre) |
| Gynecological surgery | Suggests pharmacological thromboprophylaxis* | · Consider extended duration thromboprophylaxis (e.g. up to 30 days) for high risk cancer surgery |
| Cardiac or Major vascular surgery | Suggests pharmacological thromboprophylaxis or no pharmacological thromboprophylaxis | · Follow institutional thromboprophylaxis policies· May not apply to patients at higher risk for VTE |
Objective Four:
Utilize investigations for DVT allowing for their limitations (e.g., Ultrasound and D-dimer).
Physical Exam
A JAMA Internal Medicine article from 1998 tried to assess how useful these findings were. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/210568
They found:
– The most sensitive were:
o Calf pain – Sn of 0.90
o Calf tenderness – Sn 0.84
– The most specific were:
o Superficial venous dilation – Sp 0.82
o Lowenberg sign – Sp 0.85
o Palpable cord – Sp 0.98
However, its important to recognize that even then they found that even in ‘highly suspected’ groups in the paper, the accuracy of clinical exam was an abysmal PPV of 0.55 and NPV of 0.66.
D-Dimer
Is very sensitive, but not specific at all. Meaning, if there is clotting going on, it will be elevated, but this could be anything, not just a DVT. Such as inflammatory disease, cancers, being pregnant, recent surgery, hospitalization, traumas, being older.
See? not great.
– Because of this high sensitivity, D-dimer is useful to rule OUT a VTE.
– But when it’s positive, it isn’t very useful, because for all we know, one of these other conditions is going on.
There is fairly common use of age-adjusted D-dimers with recognition that the baseline level tends to get higher with years on earth, but just know they have not been as well validated. This is done for patients older than 50 years of age but adding (age over 50 x 10 ug/L) to the upper limit of normal. Maybe it is validated https://www.mdcalc.com/age-adjusted-d-dimer-venous-thromboembolism-vte#evidence just for VTE in general focused on PE?
Compressive Ultrasound
This is the use of ultrasound to identify the presence of veins in the limb with clot in them. In the lower limb, the focus is on the popliteal veins (behind the knee) and the femoral vein (in the groin) because the branching of the veins in this area make them much more likely locations for clots to form.
The ultrasonographer will identify the vessels, sometimes they will see hyperechoic clot directly, otherwise they will try to squish the veins. Normally veins squish easily, but if there is a clot you will not be able to collapse it.
Because of this somewhat selective area of the study, if you’re still clinically suspicious of a DVT you should get a d-dimer, and if it is positive, you should repeat the study in 5-7 days, or consider requesting a whole leg study be done.
Objective Five:
In patients with established DVT, use oral anticoagulation appropriately, (e.g., start promptly, watch for drug interactions, monitor lab values and adjust dose when appropriate, stop warfarin when appropriate, provide patient teaching).
There are four anticoagulation classes available for your patient with DVT. These are DOACs, Low Molecular Weight Heparins, Unfractionated Heparins, and Warfarin.
DOACs
Generally speaking, most guidelines are going to suggest a DOAC monotherapy, due to ease of administration, no lab monitoring requirements, and comparable anticoagulation benefit with less bleed risk compared to traditional therapies.
Both Apixaban and Rivaroxaban can be initiated as monotherapy, while Dabigatran and Edoxaban require a 5-10 day LMWH course prior to initiating.
As the Xa in the name of three of these meds suggest, they act by blocking clotting factor Xa.
A quick review of dosing for the two more common DOACs:
- Apixaban (“Eliquis”) is
- 10mg PO BID for seven days, then
- 5mg PO BID for the remainder of the treatment period
- Rivaroxaban (“Xarelto”) is
- 15 mg PO BID for first 21 days, then
- 20mg PO once daily for remainder of treatment period
For each, caution with renal function less than 30mL/min and they are contraindicated in pregnancy or when breastfeeding.
LMWH
Can be considered as monotherapy for the full treatment duration, particularly for patients with active cancer, and those who are pregnant.
An important aspect is educating and reassuring on self injection. Ensuring you coach them through at least their first injection.
LMWH is most often used in conjunction with Warfarin. It is given alongside the Warfarin for at least the first five days, until the INR is 2.0 or longer for two consecutive days to prove therapeutic anticoagulation.
DVT treatment dosing for a few common LMWHs are:
- Tinzaparin – 175 units per kg SC daily
- Enoxaparin – 1.5mg per kg SC daily, or can split it into 1mg per kg BID
- Dalteparin – 200 units per kg SC daily or, for patients over 100kg, consider 100 units per kg SC BIDLow molecular weight heparin is cleared renally so generally use caution if renal function is less than 30 mL/min
Unfractionated Heparin
There are only specific cases where you might consider unfractionated heparin alone for a DVT, these include:
1. Patients with severe renal insufficiency, making other options contraindicated
2. Patients with high bleed risk, where rapid reversal of anticoagulation might be needed
3. A patient who develops a DVT shortly after receiving thrombolytic therapy
Dosing of unfractionated Heparin for a DVT:
- IV bolus 5000 units, or 80 units per kg
- Then, infusion of 18-20 units per kg per hour
- Targeting an activated partial thromboplastin time(aPTT) or anti Xa level per hospital policy
Alternatively, if using subcutaneous delivery:
- 333 units per kg initial dose
- Then, 250 units per kg BID
- This method does not require aPTT monitoring/targeting
Finally, Warfarin
As noted earlier, Warfarin treatment requires a concurrent treatment with low-molecular-weight-heparin to bridge until the Warfarin is proven therapeutic INR of 2.0-3.0. This is usually at least 5 days of LMWH bridging.
There is variability depending on the clinician on how to do this. The recommended initiation process from Lexicomp will be included in the shownotes, but looks like this:
Warfarin
- 5mg once daily initial dosing
- If elderly, frail or low body weight, consider 2-3mg per day
- If young, healthy or larger, consider 7.5-10mg per day
- Get an INR before the 4th dose of warfarin
- If INR is still under 1.5, then increase 5mg dose to 7.5-10mg daily and check again in 2-3 days
- If INR is 1.5-1.9, then continue 5mg daily and check again in 2-3 days
- If INR is 2-3, then go to 2.5mg daily and check again in 2-3 days
- If supratherapeutic but under 4.0, then drop to 1.25mg daily and check again in 2-3 days
- If INR is over 4, hold Warfarin until back under 3.0
Of course this approach is slightly different numbers if you started with higher or lower dose because of age, weight, etc. So check out the table to get the idea of how to check and adjust.

Objective Six:
Consider the possibility of an underlying coagulopathy in patients with DVT, especially when unexpected.
Anytime you diagnose a VTE, whether DVT or PE, the next words should be whether it is provoked or unprovoked.
Some provoking cause of DVT include:
- Venous trauma:
- Mechanical trauma
- Surgeries, especially orthopaedic
- Immobility:
- In-patient hospitalization
- Post-surgery
- Prolonged travel, thinking of long plane trips or long road trips
- Physiologic causes:
- Cancer
- Pregnancy
- Advanced age
- Previous DVTs
- Oral contraceptives use
- Hormone replacement therapy
- Genetic conditions
As such, if you’re not able to identify any of these as likely causes, you owe your patient some investigations to see why they developed a clot seemingly out of nowhere.
Few of the more common conditions that might be floating in your mind are: Factor V Leiden, Prothrombin gene mutation, Antiphospholipid antibody syndrome, or Deficiency of protein C and/or protein S and/or Antithrombin.
The take away from this though it that generally this workup is not the purview of the GP. There is quite a lot of nuance in the diagnosis, testing interpretation and so on, so if it is available the recommendation is to refer to your friendly Haematologist or Thrombosis clinic if available to you if you have recurrent or unprovoked VTEs.
Objective Seven:
Use compression stockings in appropriate patients, to prevent and treat post-phlebetic syndrome.
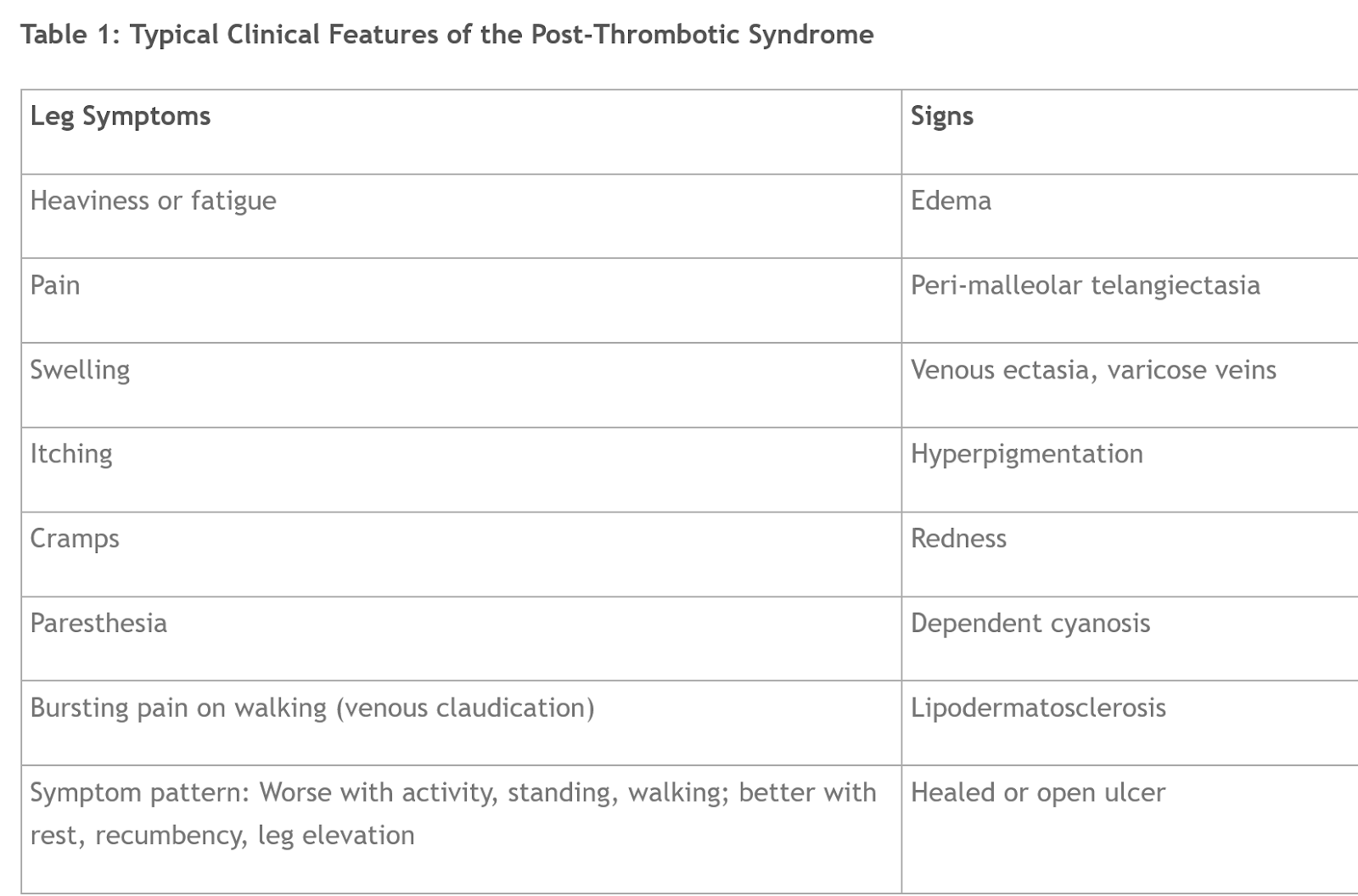
This is a chronic condition that develops in up to 50% of patients after DVT treatment. It’s a clinical diagnosis, based on some symptoms we will mention and usually waiting until 3-6 months after DVT resolution before diagnosing. There is a scoring system, but we’ll put that in the shownotes in case it is of interest to you
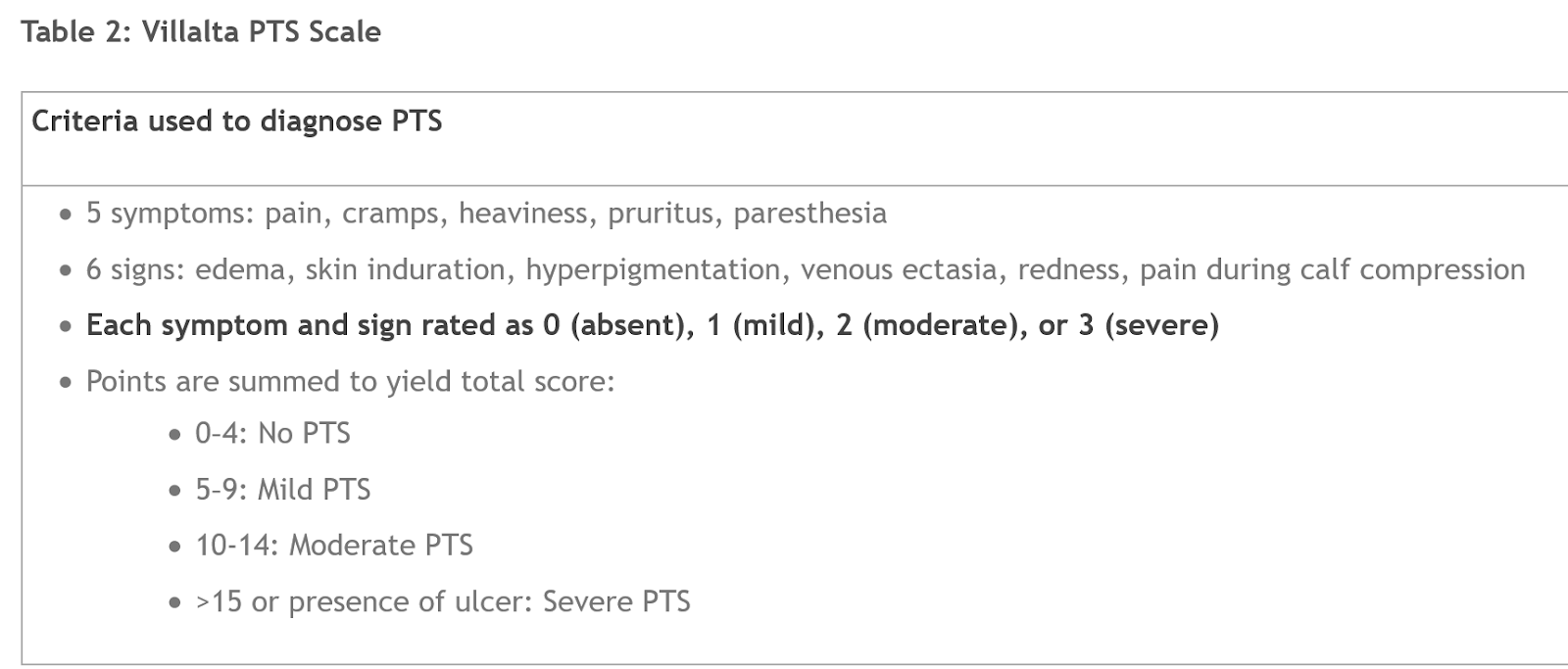
I hadn’t heard of it before, so a quick review of what the symptoms of post-thrombotic syndrome might look like clinically:
A Cochrane review4 reported that compression stockings (30–40 mm Hg) used early after the diagnosis of DVT were associated with a 69% reduction in the odds of postthrombotic syndrome developing and a 61% reduction in the odds of severe postthrombotic syndrome.
However, a recently concluded trial did not show a benefit to using external compression stockings as a preventive measure.5 for up to 24 months. So, I hope they update this objective to reflect this new evidence.
Alternatively to compression stocking, a systematic review showed that long-term treatment with low-molecular weight heparin after DVT resulted in a lower incidence of postthrombotic syndrome than treatment with anticoagulants administered orally.6 There is currently no evidence from randomized controlled trials to support the role of thrombolysis in preventing postthrombotic syndrome
Thrombosis Canada has a quick summary of available options for these patients, with the focus on prevention of PTS, and some symptomatic options if they do get this:

Resources Used
1. Thrombosis Canada 2020 Clinical Guides – https://thrombosiscanada.ca/clinicalguides/#
2. Tintinalli’s 8th Edition, Ch 56 pp 391-394
3. https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2105684.

Great review, but I think you guys should include the info from this as well!: https://veinscarolina.com/understanding-the-difference-between-phlebitis-and-dvt/
Hi Chaminda,
Great point!
This post was intended to cover the objectives from the CCFP, which sometimes misses some of the nuance around these.
No doubt differentiating SVT/Phlebitis from DVT is important and would be identified on compressive ultrasound.
If we get a chance to do a General Practice episode on these that doesn’t focus on the specific objectives of the CCFP we definitely will.
As a local resource I might point to the Thrombosis Canada https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=90
Awesome, thanks so much! You guys are amazing!