
- Written & Researched By: Khash Farzam
- Peer Review By: Caleb Dusdal
Objective One:
In all patients presenting with symptoms of prolonged or recurrent cough, dyspnea, or decreased exercise tolerance, especially those who also have a significant smoking history, suspect the diagnosis of chronic obstructive pulmonary disease (COPD).
COPD is a form of obstructive lung disease with the classic symptoms of cough, shortness of breath and sputum production. Smoking is considered by far the number one risk factor for developing COPD. Other risk factors for specifically COPD, can include exposure to various pollutants that can be inhaled.
The typical patient will generally be a former smoker or current smoker, has had a chronic progressive cough and progressive shortness of breath that may or may not be limiting their ability to function.
The symptoms of new onset shortness of breath and cough generally can overlap with other serious conditions, especially in patients who do not have a prior diagnosis of COPD. Congestive heart failure and acute coronary syndrome can both present similarly to undiagnosed COPD and share smoking as a common risk factor.
In the absence of chest pain and a euvolemic volume exam in these patients, COPD generally becomes the most likely diagnosis but the general point is that one must be mindful of cardiac and respiratory etiologies with the same symptoms and rule them out when appropriate. Pneumonia can also have a similar presentation, though often is accompanied by a fever. Of course, COVID will always be on our differential for any exacerbated COPD symptoms.
Objective Two:
When the diagnosis of COPD is suspected, seek confirmation with pulmonary function studies (e.g., FEV1).
The first line test in establishing the diagnosis of COPD in the outpatient setting, is spirometry testing.
The purpose of this test is to assess the degree of airway obstruction. It looks at a few different things to establish the diagnosis of COPD. Two key components are the FEV1 and FVC.
The FEV1 is the “forced expiratory volume in one second.” As the phrase suggests, it is how much air can be breathed out by the patient in the first second of their breath.
On the other hand, FVC stands for forced vital capacity. Quite similar to FEV1, it looks at the total volume of air that can be expelled in a large single breath.
The FEV1 and FVC are compared in a ratio format and if someone is <70%; they likely have an obstructive airway disease, the most common of which is COPD.
An additional criteria to consider and incorporate is the DLCO which is the diffusing capacity of carbon monoxide. Those with COPD with emphysema tend to have lower DLCO and this helps supports the diagnosis.
If a patient who exhibits symptoms of COPD, does not meet diagnostic criteria on the spirometry, then it’s important to investigate for other causes such as heart disease and pulmonary hypertension. And other things to include on the differential diagnosis include:
- bronchiectasis,
- tuberculosis,
- asthma,
- obliterative bronchiolitis and
- diffuse panbronchiolitis.
Evaluation for these other entities depends on the patient’s demographics, symptoms and risk factors.
Of note, during spirometry testing there shouldn’t be much reversible change in the FEV1 and FVC after administration of inhaled salbutamol, whereas in asthma there is significant reversible change.
One perk to keep in mind, early-onset COPD, COPD without a smoking history that has other similar diagnoses excluded, or simultaneous COPD with unexplained transaminitis, would warrant alpha 1 anti-trypsin testing. While uncommon, this traditionally was considered a very rare diagnosis due to undertesting but is now more commonly diagnosed.
Objective Three:
In patients with COPD, use pulmonary function tests periodically to document disease progression.
Table 2. Levels of severity in COPD1,6
| COPD Severity | Symptoms | FEV1 (% predicted) | History of exacerbations | Comorbidities |
| Mild | – Breathlessness on moderate exertion – Recurrent chest infections – Little or no effect on daily activities | ≥ 80 | Frequency increases with severity | Exist across all severity levels (e.g., cardiovascular disease, skeletal muscle dysfunction, metabolic syndrome, osteoporosis, anxiety or depression, lung cancer, peripheral vascular disease and sleep apnea) |
| Moderate | Increasing dyspneaBreathlessness walking 100 m on level groundIncreasing limitation of daily activitiesCough and sputum productionExacerbations requiring corticosteroids and/or antibiotics | 50 – 79 | ||
| Severe | Dyspnea on minimal exertion Daily activities severely curtailed Expiring regular sputum production Chronic cough | 30 – 49 | ||
| Very severe | < 30 |

Objective Four:
Encourage smoking cessation in all patients diagnosed with COPD.
Quitting smoking is by far one of the most important things patients can do to improve their survival and life expectancy. Despite all of the advancements made in modern medicine and novel respiratory treatments, there are just two things that can improve life expectancy for COPD: oxygen support therapy and smoking cessation.
Physicians should engage as often as possible with their COPD patients (and even smoker non-COPD patients!) to explore treatment avenues that help with smoking cessation.
This is not the smoking cessation episode, so we won’t go into depth here, but know about Varenecline, Wellbutrin, and Nicotine replacement therapy.
Objective Five:
Offer appropriate vaccinations to patients diagnosed with COPD (e.g., influenza/pneumococcal vaccination).
We are very comfortable with the term “COPD exacerbation” given how common of an admitting diagnosis it is. But seldom do we ask, why is this patient having an exacerbation? There is generally a trigger of some sort.
Influenza and other upper and lower respiratory infections can be a common trigger of COPD exacerbations. Hence, we need to make sure our patients with COPD are getting their annual flu shots on time. In addition, the Pneumococcal polysaccharide 23-valent vaccine (also known as Pneumovax) is indicated for all COPD patients as well as the pneumococcal 13 vaccine (known as Prevnar).
Of course, we can likely expect that COVID vaccination will also become a key component of preventative care of the COPD patient.
Objective Six:
In an apparently stable patient with COPD, offer appropriate inhaled medication for treatment (e.g., anticholinergics/bronchodilators if condition is reversible, steroid trial).
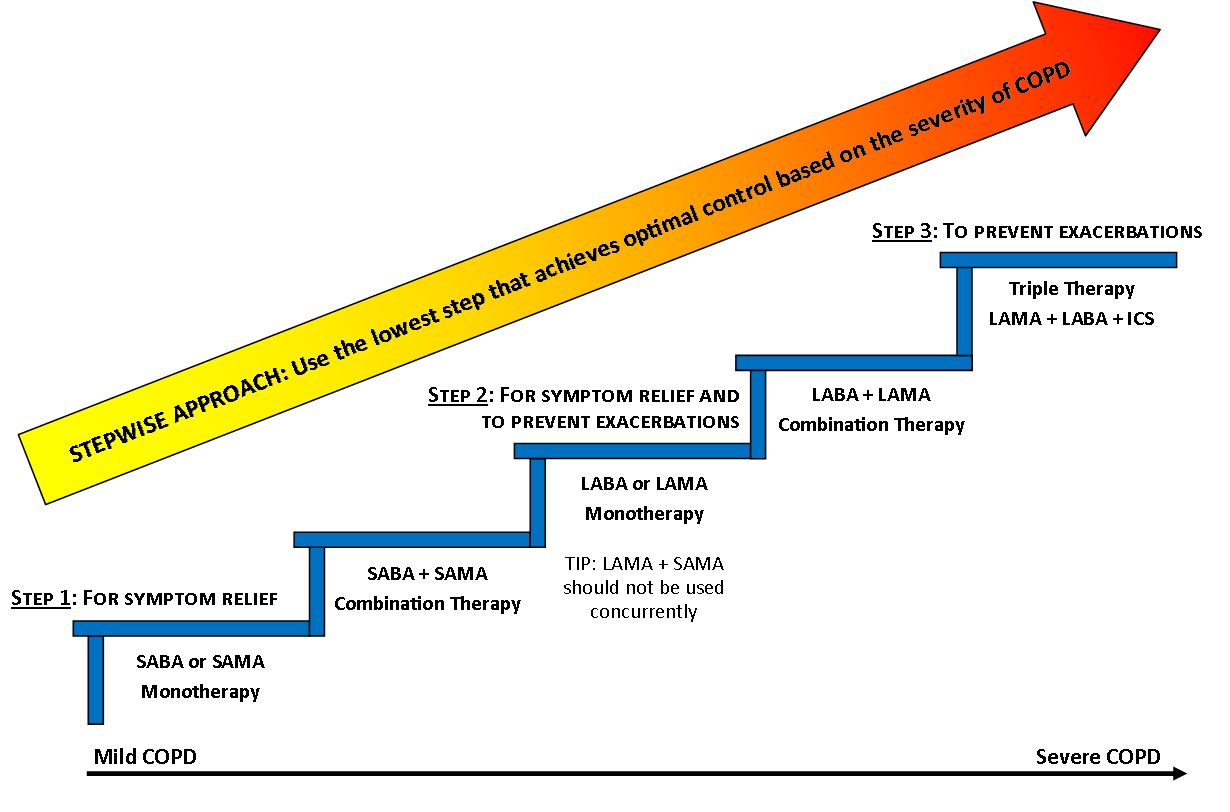
Similar to asthma, COPD treatment follows a stepwise approach. Mild COPD patients can often be managed well with a short acting beta agonist inhaler. Often, they will use it as needed up to daily use. For mild COPD, step one is focused on symptom relief.
As severity progresses, there is a focus on both symptom relief and preventing exacerbations. At this step, introduction of a SAMA inhaler for combination therapy is necessary. The general principle is that longer acting is more clinically potent than short acting. So as disease progression occurs, utilization of a LABA and LAMA is quite common as monotherapies. Most patients eventually have combination therapy inhalers LABA and LAMAs along with an as needed SABA.
Use of inhaled steroids is often used in more advanced COPD in combination with a LABA and LAMA for triple therapy.
Interval assessment of disease severity on an outpatient basis is required as it allows for escalation of therapy. For a deep dive into all of the evidence on these therapies, check out the recent 3-part podcast series by Best Science Medicine who go into all of the details. Suffice it to say that many of these therapies for more advanced COPD have very small benefits.
Oral steroids (and possibly IV steroids) have a major role in treating COPD exacerbations. A 5 day course of steroids if routinely given to patients experiencing an exacerbation, with prednisone (50mg daily for 5 days) being the favored choice though some institutions may prefer IV methylprednisolone.
Antibiotic use for COPD exacerbations are often debated. Many institutions will favor using a macrolide course of antibiotics for their added anti-inflammatory effects and possible bacterial component of the COPD exacerbation. The primary benefit seen is around reduced length of stay. Exacerbation treatment will also always include a SAMA and SABA combination therapy, generally in nebulized form in set intervals.
Always remember to involve your patient in their own health as well. One way to do this is to incorporate a patient COPD flare up action plan, which we will link to in the show notes.

Objective Seven:
Refer appropriate patients with COPD to other health professionals (e.g., a respiratory technician or pulmonary rehabilitation personnel) to enhance quality of life.
Patients experiencing moderate to severe COPD are good candidates for pulmonary rehab. The respiratory workers generally work with patients on various general exercises to help improve respiratory health. They also can help teach patients breathing exercises to help their symptoms.
For COPD a key intervention our multidisciplinary colleagues can offer is Pulmonary Rehabilitation. This generally looks like, 4-12 weeks with sessions lasting 2-3 hours a few times per week. Most often in hospital, but community programs are also done.
A Cochrane systematic review in Feb 2015 covered 65 RCTs comparing usual care to pulmonary rehab for these folks with COPD and found improvement in essentially every measures that they tracked: functional exercise capacity, dyspnoea, fatigue, emotional function, https://www.cochrane.org/CD003793/AIRWAYS_pulmonary-rehabilitation-for-chronic-obstructive-pulmonary-disease
However, despite this evidence, a survey of every hospital in Canada published in 2015 showed that somehow only an estimated 0.4% of patients with COPD had access to a pulmonary rehabilitation program https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4470547/
Objective Eight:
When treating patients with acute exacerbations of COPD, rule out co-morbidities (e.g., myocardial infarction, congestive heart failure, systemic infections, anemia).
A typical patient having a COPD exacerbation presents with shortness of breath as a key symptom. Like everything else in medicine, there is always overlap in symptoms and diagnoses. Many COPD patients also suffer from some form of cardiac disease, often due to the shared cardiac risk factor of smoking history. Other common diagnoses that must be considered are pneumonia (often includes cough and sputum production) and pulmonary embolisms.
When presented with a patient who has likely COPD exacerbation, assessment of vital signs are a key first step. Checking an oxygen saturation and seeing that the patient is hypoxic is generally a good indication that the patient needs to be sent to the emergency room (if they’re being seen in clinic) or that they likely require admission if they’re being evaluated in the emergency room. A patient who is febrile is logically concerning for infection but also PE if it’s a low grade fever.
The physical exam in a COPD patient can be very useful in differentiating COPD exacerbation from CHF if the patient has a history of both diagnoses (quite common!). It also helps us make the clinical assessment of pneumonia. The respiratory exam specifically, may be somewhat less revealing if one is suspecting PE though.
The most useful physical exam findings include:
- Early inspiratory crackles – LR 14.6
- Absent cardiac dullness at left lower sternal border – LR 11.8
- Breath sound score of 9 or less – LR 10.2
- involves listening over three spots on each lung and scoring the inspiratory sound as either:
- absent(0 points),
- barely audible(1 point),
- faint but definitely heard(2 points),
- normal(3 points) or
- louder than normal(4 points)
- involves listening over three spots on each lung and scoring the inspiratory sound as either:
- Subxiphoid cardiac impulse – LR 7.4
- Hyperresonance of the chest – LR 7.3
- others with slightly lesser likelihood ratios include
- Hoover sign (this is inward movement of the lower rib care with inspiration, rather than the normal outward flare, as a result of a flat but functioning diaphragm)
- Forced expiratory time greater than 9 seconds
- Maximum laryngeal heights <= 4cm
- use of sternocleidomastoid or scalenes for breathing




The typical COPD patient will have diffuse bilateral wheezing on auscultation and tend to have a euvolemic volume assessment exam. In contrast, the CHF patient will have bibasilar crackles on auscultation and be notably hypervolemic. Of course, simultaneous flare ups are always possible and treating hypervolemia is always favorable for improving respiratory status.
So what tests to order? Since the differential diagnosis for shortness of breath is broad (even if accompanied by cough and increased sputum production) – starting labs will generally include a CBC, CMP, BNP, troponin and a blood gas.
Our CBC will tell us if there is any leukocytosis while also ruling out major anemia. BNP is quite useful especially if prior BNP levels are known for the specific patient. It helps give an objective assessment of volume status in CHF patients. It is limited by the fact that it is falsely low in very obese patients.
The troponin is one of our main tools for ruling out an acute coronary syndrome for the undifferentiated patient. And our blood gas can do a good job of almost ruling out COPD exacerbation if the patient has a completely normal CO2 since COPD patients tend to retain CO2. It can also tell us if the patient is doing worse than they clinically appear (if there is any acidosis).
If there is some suspicion of PE, a d-dimer can be obtained as a step to rule out a blood clot. Alternatively, a high suspicion for PE warrants a CT angio of the chest. Listen to Chest Pain part 2 for a more thorough discussion of the workup and management.
Simultaneous to our lab tests, an EKG and chest x ray are also obtained. The EKG is part of the cardiac evaluation. The chest x ray can show signs of pulmonary edema, pneumonia and some signs of emphysema such as hyperinflation.
Once the workup has been done, the patient can proceed to be treated for a COPD exacerbation. It’s quite important to complete the comprehensive evaluation since mild to moderate COPD exacerbations can often resemble other acute cardiorespiratory disease exacerbations. Of course, in the era of COVID; a covid rule out will also be done.
Objective Nine:
In patients with end-stage COPD, especially those who are currently stable, discuss, document, and periodically re-evaluate wishes about aggressive treatment interventions.
Patients who have end stage COPD generally may qualify for hospice and palliative care management. Often patients are on near-maximum levels of home oxygen along with stage 4 symptoms and other clinical criteria. The primary goal at that stage would be maximizing quality of life and managing symptoms.
If you want to brush up on this a little bit, refer back to episode ten ‘Bad News’ particularly the resources for that episode such as the ‘Difficult Conversation Guide’. Whenever these discussions happen, it’s very important to emphasize to the patient that these decisions can be changed at any time. That helps prevent patients from feeling like they’re signing away on what to do in that very moment with no return and limited time to think.
We will be including the general steps from the LEAP palliative course in the shownotes and recommend you also take a course similar to this as these conversations are most likely to take place with their family physician(you!) Its important to recognize that end stage COPD is progressive and should be a prompt to have this conversation with your patient.


One thought on “CCFP Topic: COPD”