
- Written/Researched By: Caleb Dusdal
- Reviewed By: Dr. Abid Khattak & UBC Resident Sophia Park
Objective One
For a patient with multiple unexplained symptoms or behaviours, look for anxiety as a primary or contributing cause.
Many patients may present with one or more symptoms that are not explained or attributable to a specific medical diagnosis. These can include the sympathetic symptoms such as palpitations, shortness of breath, hyperventilation, sweating and chest pain or other somatic symptoms like abdominal pain, dyspepsia, chest pain, fatigue, dizziness, insomnia, and headache. While some of these are included in our favourite screening tool, the GAD7, not all of them are, and you will still need to think about anxiety when seeing a patient with one of these complaints.
The GAD-7 is a screening tool, it is not diagnostic, and can be used for tracking the severity of anxiety. The GAD7 includes the following questions:
Over the past two weeks, how often have you been bothered by the following occurrences:
- Feeling nervous, anxious, or on edge?
- Not being able to stop or control that worry?
- Worrying too much about multiple different things
- Having trouble relaxing?
- Being so restless you have difficulty sitting still?
- Being easily annoyed or irritable?
- Feeling afraid as if something awful might happen?
For each question, score as follows:
- ‘not at all’ = 0 points
- ‘several days’ = 1 point
- ‘more than half the days’ = 2 points
- ‘nearly every day’ = 3 points
A score of 5-9 suggests mild anxiety, a score of 10-14 is moderate anxiety, and 15 or more points suggests severe anxiety disorder.
Objective Two
When a patient presents with symptoms of anxiety, clearly distinguish between distress (e.g. fear, nervousness, worry) and an anxiety disorder.
Anxiety is a normal physiologic response to events in life. Evolutionarily, this trigger for catecholamines might make the difference in escaping from a crazed warthog or not. This is distress and may be appropriate for the patient’s circumstance and needs to be explored.
This becomes a disorder, when the anxiety causes clinically significant distress, or functional impairment. Such as from being excessive for an otherwise benign trigger, or generalized anxiety about imagined or inconsequential concerns.
Objective Three
In a patient presenting with acute symptoms of panic (e.g., shortness of breath, palpitations, hyperventilation), do not attribute the symptoms to anxiety without first excluding serious medical pathology (e.g., pulmonary embolism, myocardial infarction) from the differential diagnosis, especially in patients with established anxiety disorder.
This can be a daunting undifferentiated patient to have arrive into your emergency department or clinic. Particularly if they already have a documented anxiety or panic disorder. The struggle is that a lot of the sympathetic symptoms, such as palpitations, shortness of breath, hyperventilation, sweating and chest pain carry a ton of overlap with conditions that should make your sphincter tighten.
Depending on what the patient’s major complaint is you will want to think about the scary things that could be causing that. This is the same thing you will do every day whether you’re working in the clinic or the emerg. The only difference is that panic and anxiety are on your differential.
Objective Four
When working up a patient with symptoms of anxiety, and before making the diagnosis of an anxiety disorder,
a) Exclude serious medical pathology
b) Identify: other co-morbid psychiatric conditions, abuse, substance use
c) Assess the risk of suicide
d) Discuss functional impact with the patient
Exclude serious medical pathology
- Rule out organic causes, thinking of things like:
- Pheochromocytoma
- Hyperthyroidism
- Cardiac or Pulmonary Disease
- Central Structural Pathology
- Hypoglycemia
[Portico: Psychiatry in Primary Care: https://www.porticonetwork.ca/web/psychiatry-primary-care/clinical-situations/anxiety/differential-diagnosis ]
The Canadian Clinical Guidelines for anxiety 2014 recommend getting at least the following baseline labs for a new presentation of anxiety:
- CBC
- Fasting lipid profile
- Fasting glucose
- Electrolytes
- Thyroid stimulating hormone
- Liver enzymes
- If warranted, urine toxicology for substance use
Other comorbid psychiatric conditions
This is important because Generalized Anxiety Disorder is associated with high psychiatric comorbidity, including other anxiety disorders and major depressive disorder.
Here we might benefit from always remembering to, by default in a psychiatric interview, do a psychiatric functional screen, remembered by the acronym MOAPS:
M – is for mood, including manic episodes
- screen for depression, such as with PHQ-2
- Over the past two weeks how often have you felt little interest in doing the things you used to enjoy?
- Over the past two weeks how often have you felt down, depressed or hopeless?
O – rganic causes
- Alcohol, drugs or delirium
A – nxiety, asking around
Excessive worry, obsessions, compulsions, or panic attacks
P – sychosis
- Have you been seeing or hearing things that other people don’t see or hear?
- Do you have deeply held beliefs that no one else around you believes are true?
S – uicidality
- Ask about ideation, plans and prior attempts
Substance Use
ubstance use
A few key substances to consider that can cause symptoms of anxiety are:
- Amphetamines, cocaine, or
- Withdrawal from EtOH or Benzodiazepines
- New use of marijuana can also cause anxious symptoms
Screen for suicidality
Anxiety and related disorders are independently associated with an up to 2.5x risk of suicide attempts.
Within the specific anxiety disorders, increased attempts and completed suicides are higher among patients with:
- PTSD
- Panic disorder, and
- Generalized Anxiety Disorder
And the presence of a co-morbid mood disorder significantly increases this risk of suicide even more.
As such, we should be sure to assess all of our patients with, or suspected of having, anxiety disorder:
- Have you recently felt as though your life is not worth living?
- Have you thought about hurting yourself?
- Have you thought of killing yourself?
- Did you have a specific plan and planned time to kill yourself?
A common Mnemonic for risk factors for suicide is SAD PERSONS. We couldn’t uncover any great validation evidence for the tool, a good sized trial published in 2017 found it to have a sensitivity of only 49% and specificity of only 60%. But it is very commonly referred to and so may be useful from an exam perspective.
- Sex is male
- Age is over 45
- Depression
- Previous attempts
- Etoh abuse
- Rational thinking loss
- Separated, widowed or divorced
- Organized plan
- No social supports
- Stated future intent
Functional impact due to anxiety disorder
- Social. How does their anxiety affect seeing and keeping friends?
- Work. Have they missed work, or been punished or has their work suffered as a result of their anxiety?
- School. Have they missed any school as a result of their anxiety?
Objective Five
When an anxiety disorder is suspected, assess and classify according to established diagnostic criteria, as treatment will vary according to the classification.
Panic Disorder
Panic Disorder
Look for:
- Recurrent and unexpected attacks, in the absence of identifiable triggers
and - Persistent concern about additional attacks with maladaptive changes in behaviour related to fear of these attacks recurring
Mnemonic for remembering a panic attack is STUDENTS Fear the 3 C’s:
- Sweating
- Trembling or shaking
- Unsteadiness, dizziness, light headed or faint
- Depersonalisation or derealisation
- Excessive heart rate, palpitations
- Nausea or abdominal distress
- Tingling (numbness or paraesthesias)
- Shortness of breath or smothering
- Fear of dying, losing control or going crazy
- 3 C’s: chest pain, chills, choking
Agoraphobia
Agoraphobia
Look for:
- Marked and unreasonable fear or anxiety about a situation
and - Active avoidance of feared situations due to ideas that escape might be difficult or help unavailable of symptoms were to occur
Remember the diagnostic criteria with the mnemonic COOPE
- Crowded area
- Open spaces
- Outside the home
- Public transport
- Enclosed spaces
Specific Phobias
Specific Phobias
Look for:
- Marked and unreasonable fear or anxiety of particular objects or situations
- Some common examples are heights, animals, injections, seeing blood, etc
Mnemonic is PHOBIA
- Persistent (>6 months)
- Handicapping (restricted lifestyle)
- Out of proportion
- Beginning immediately and almost always
- Intense fear or anxiety about a specific object or situation leading to
- Avoidance
Social Anxiety Disorder
Social Anxiety Disorder (SAD)
Look for:
- Marked, excessive or unreasonable fear or anxiety about social situations in which there is possibility of scrutiny by others
and - Active avoidance of these situations as a result
Mnemonic is FEARED:
- Fear of social situations where exposed to possible scrutiny by others; Fears of being negatively evaluated
- Exposure to the social situation almost always provokes fear or anxiety
- Avoids the social situation or endured with intense fear or anxiety
- Recognises that the fear is out of proportion
- Exclusion of fear induced by a substance or another mental or medical disorder; Excessive/unrelated to fear of another coexisting medical condition
- Distress or impairment; Duration lasting for 6 months
Generalized Anxiety Disorder
Look for:
- Excessive and difficult to control anxiety and worry about multiple everyday events or activities
- Accompanied by restlessness, feeling on edge, or muscle tension
Mnemonic is WATCHERS
- Worry and Anxiety
- Time for at least 6 months
- Controlling the worry difficult
- Handicapping
- Exclude another mental disorder
- Rule out worry, not due to physiological effects of a substance or another medical condition
Obsessive Compulsive Disorder (OCD)
Look for:
- Obsessions: recurrent and persistent thoughts, urges or images experienced as intrusive and unwanted, and that cause marked anxiety
- Compulsions: repeptive behaviours, such as hand washing, or mental acts, such as counting, that the pt feels driven to perform in order to reduce the anxiety caused by the obsessions
Mnemonic is Thoughts RIDE TIME, Acts Reduce TIME: [you can probably just refer them to the show notes for this one]
- Presence of obsessions, compulsions, or both
- Obsessions: ‘Thoughts RIDE’
- Thoughts, urges or images that are:
- Recurrent and persistent.
- Intrusive and unwanted.
- Distress (anxiety) provoking
- Effaced by ignoring or suppressing or neutralising with other thought or compulsion.
- Thoughts, urges or images that are:
- Compulsions: ‘Acts Reduce’
- Acts, mental or behavioral, repetitively performed in response to an obsession or according to rigid rules.
- Reduce or prevent anxiety or distress, prevent a dreaded event.
- Obsessions: ‘Thoughts RIDE’
- Time-consuming or IMpair socio-occupational functioning.
- Exclude being induced by a substance or another medical condition.
- Exclude another mental disorder.
Post-Traumatic Stress Disorder (PTSD)
Look for:
- Exposure to an actual or threatened death, serious injury or sexual violation
- Intrusive symptoms are present, such as distressing memories, dreams, flashbacks
And
Avoidance of stimuli associated with the traumatic event
and
Negative alterations in cognition and mood as well as marked alteration in arousal and reactivity, which look like irritable behaviour and/or hypervigilance
Mnemonic is TRAAUMA:
- Traumatic event: witnessed or experienced or occurred to dearest or exposure repeatedly to its aversive details
- Re-experience one of following intrusion symptoms: memories, nightmares, flashbacks, psychological distress or physiological reaction to cues symbolising the traumatic event
- Avoidance of memories, thoughts, feelings of the traumatic event or its reminders
- Alterations in cognitions and mood negatively:
- forgetting, mislabelling, blaming, no positive emotions, always negative emotions, anhedonia, detachment (two of seven)
- Unable to function or cause distress/Unattributed to a substance or another medical condition
- Month or more of symptoms
- Arousal and reactivity increased with two of the following:
- irritability,
- recklessness,
- hypervigilance,
- startling,
- concentration and
- sleep disturbances
Objective Six
In patients with known anxiety disorders, do not assume all new symptoms are attributable to the anxiety disorder.
This is a vital point.
It becomes very easy to see ‘Anxiety’ on a patient’s medical history and assume their new presentation is a result of this. While this should be taken into the patient’s personal context, please remember that these patients still have all of the same anatomical systems as any of your other patients, and so deserve the same clinical, lab and imaging workup you would perform for anyone else.
Objective Seven
When planning management of anxiety, offer appropriate treatment, which may include one or a combination of the following:
• Self-management techniques
• Regular office follow-up, Community resources
• Structured therapies (Cognitive Behavioral Therapy, psychotherapy)
• Judicious use of pharmacotherapy
Self-Management Techniques
Several self driven CBT based options are available to suggest to patients including apps like Mindshift from Anxiety Canada, and the bounceback websites based in BC and Ontario, but available to anyone. A number of other resources are suggested by porticonetwork, including:
- Canadian Mental Health Association, link provided in show notes
- Local mood disorders support groups, see Mood Disorders Society of Canada
- Several books are also recommended including, the feeling good handbook, mind over mood, How to break free from negative thought. Full dsetails are in the show notes, along with other associations and agencies.
- [some further online links for shownotes]
- Canadian Mental Health Association
- Canadian Network for Mood and Anxiety Treatments
- Internet Mental Health
- Mood Disorders Society of Canada
- National Institute of Mental Health
- Academy of Cognitive Therapy
- British Association for Behavioural and Cognitive Psychotherapies
- Centre for Addiction and Mental Health
Regular office follow-up
Sometimes just arranging regular follow-up appointments with your patients experiencing anxiety can be enough to support them.
Of course this can also allow you to keep a closer eye on the progress and whether more significant intervention is needed.
Judicious Use of Pharmacotherapy
Health Canada Approved medications, with guidelines recommendations in the screenshot below each condition.
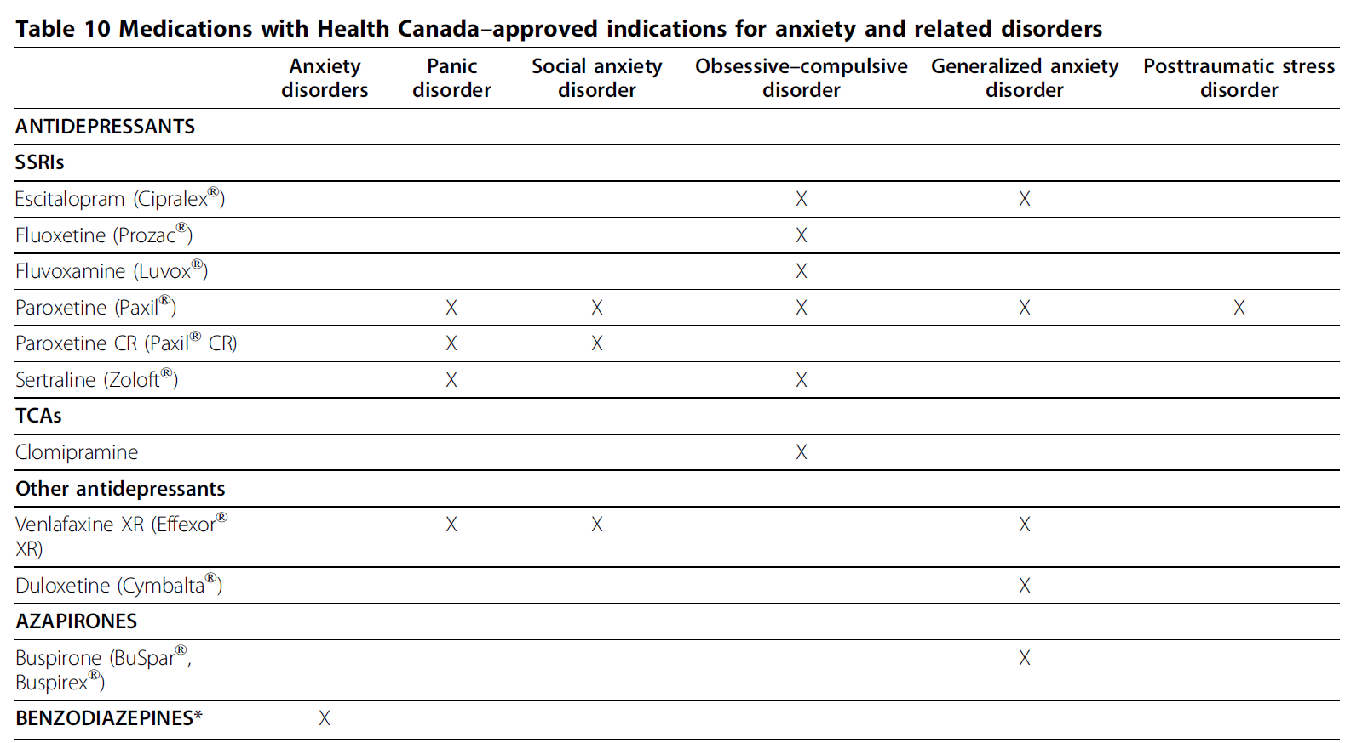
- Panic Disorder
- SSRIs
- Paroxetine
- Sertraline
- SNRI
- Venlafaxine
- SSRIs

- Generalized Anxiety Disorder
- SSRIs
- Escitalopram
- Paroxetine
- SNRI
- Venlafaxine
- Duloxetine
- Buspirone
- SSRIs

- Social Anxiety Disorder
- SSRIs
- Paroxetine
- SNRI
- Venlafaxine
- SSRIs

- Obsessive Compulsive Disorder
- SSRIs
- Escitalopram
- Fluoxetine
- Fluvoxamine
- Paroxetine
- Sertraline
- TCAs
- Clomipramine
- SSRIs

- Post-Traumatic Stress Disorder
- SSRI
- Paroxetine
- SSRI

Referral to other health professionals with ongoing shared care
Depending on your local circumstance this might look like:
- Psychologist with CBT training
- Social worker or RN with CBT training
- Counsellors
- Some PCNs have adult mental health non-urgent and urgent outpatient clinics
Objective Eight
When managing anxiety or an anxiety disorder do not use medication as a sole treatment.
A 2011 meta-analysis found that on balance there was no significant difference in the benefits of CBT compared to pharmacotherapy for anxiety disorders.
Although there was some difference for specific anxiety disorders, for example, BCT was favoured for panic disorder, no real differences were seen for OCD and seasonal affective disorder.
Of course, given the relatively little risk of side effects from CBT, this should be your first intervention for a patient presenting with anxiety or an anxiety disorder. The struggle is likely to be access to CBT professionals. There are practitioners who are trained in CBT, but the waitlist can often be quite long, and if you are not in an urban centre the availability becomes even less.
Objective Nine:
When assessing and managing anxiety, discuss the use of alcohol and substances as harmful self-medication.
First, it is important to recognize that this is unhelpful for a patient who is not interested in quitting smoking, alcohol or drug use. However, you should use every point of contact as an opportunity to ask them about their degree of interest in quitting.
Recognize that these are often used as self-medication by persons suffering from mental health disorders such as anxiety.
References Used:
[1] Comer JS, Blanco C, Hasin DS, Liu SM, Grant BF, Turner JB, Olfson M: Health-related quality of life across the anxiety disorders: results from the national epidemiologic survey on alcohol and related conditions (NESARC). J Clin Psychiatry. 2011, 72: 43-50.
[1] Nepon J, Belik SL, Bolton J, Sareen J: The relationship between anxiety disorders and suicide attempts: findings from the National Epidemiologic Survey on Alcohol and Related Conditions. Depress Anxiety 2010, 27:791-798.
Cougle JR, Keough ME, Riccardi CJ, Sachs-Ericsson N: Anxiety disorders and suicidality in the National Comorbidity Survey-Replication. J Psychiatr Res 2009, 43:825-829.
Pfeiffer PN, Ganoczy D, Ilgen M, Zivin K, Valenstein M: Comorbid anxiety as a suicide risk factor among depressed veterans. Depress Anxiety 2009, 26:752-757
[1] Katz C, Randall JR, Sareen J, Chateau D, Walld R, Leslie WD, Wang J, Bolton JM. Predicting suicide with the SAD PERSONS scale. Depress Anxiety. 2017 Sep;34(9):809-816. doi: 10.1002/da.22632. Epub 2017 May 4. PMID: 28471534.
iv. Mnemonics for diagnostic criteria of DSM V mental disorders: a scoping review General Psychiatry 2020;33:e100109. doi: 10.1136/gpsych-2019-100109
[1] Roshanaei-Moghaddam B, Pauly MC, Atkins DC, Baldwin SA, Stein MB, Roy-Byrne P: Relative effects of CBT and pharmacotherapy in depression versus anxiety: is medication somewhat better for depression, and CBT somewhat better for anxiety? Depress Anxiety 2011, 28:560-567.
[1] Bandelow B, Seidler-Brandler U, Becker A, Wedekind D, Ruther E: Metaanalysis of randomized controlled comparisons of psychopharmacological and psychological treatments for anxiety disorders. World J Biol Psychiatry 2007, 8:175-187.
Portico Network: Psychiatry in Primary Care https://www.porticonetwork.ca/
Canadian Clinical Practice Guidelines on the management of anxiety, PTSD and OCD. https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-14-S1-S1
Thank you very much for this amazing podcast. Where are the show notes? Some of the topics don’t have the show notes available.
Ya, something blew up on the backend and they disappeared, we’re gradually replacing them. Sorry for any inconvenience.